
The Science of Longevity: What You Should Know Today—and Where We Are Going
By Stefano Sinicropi, M.D, FAAOS | Spine Surgeon | Longevity Expert | Author of Wellness at the Speed of Light | Founder, HyperCharge Health | Co-Founder, Above Genetics
Medical Disclaimer: This white paper is intended for educational purposes and does not constitute medical advice. The information contained herein reflects the clinical perspective of Dr. Stefano Sinicropi and the research team at HyperCharge Health and is not a substitute for individualized medical consultation. GHK-Cu and related peptide compounds should only be used under the supervision of a qualified healthcare provider. Individual results will vary. As with any therapeutic intervention, risks and benefits must be evaluated in the context of each patient’s specific medical history, current medications, and treatment goals.
We are the first generation of physicians with the tools to ask a once-unthinkable question: not merely how to treat the diseases of aging, but whether aging itself can be slowed, measured, and—in the laboratory, already—reversed.
Executive Summary
For all of human history, aging has been treated as fate—a one-way road that bends, inevitably, toward frailty. Medicine has organized itself around that assumption. We wait for disease to appear, then we manage it: a pill for the blood pressure, a stent for the artery, a procedure for the spine. We have become extraordinarily good at managing decline and surprisingly poor at preventing it.
This white paper argues that the assumption is wrong—and that the science to prove it wrong has arrived. Aging is not simply wear and tear. It is, at the cellular level, a controlled and increasingly measurable process. And anything that can be measured can, in principle, be managed, slowed, and in some settings reversed.
Drawing on the cellular-aging framework advanced by Michael Fossel, M.D., Ph.D., in his book Reversal, and on the practical, self-directed optimization toolkit assembled by Ben Greenfield in Boundless, this paper maps three things: where longevity science actually stands today, what you can act on right now, and where the field is heading over the next decade. I write as a spine surgeon who spent the first half of my career treating the downstream wreckage of aging—and the second half convinced that we have been intervening far too late.
The central thesis is simple: stop treating aging as a decline to be endured, and start treating it as a problem to be solved—upstream, at the level of the cell.
This is not a promise of immortality, and it is not a sales pitch for any product. It is an honest accounting of a field moving at the speed of light—and an invitation to become, as I argue throughout my work, the CEO of your own health.
Part I — Where We Are: A New Understanding of Aging
From “Wear and Tear” to a Programmed Process
The oldest theory of aging is the one most of us carry intuitively: the body is a machine, and machines wear out. Joints grind down, arteries stiffen, the brain slows. Under this model, the best we can do is replace parts and slow the friction.
The modern science of aging tells a more interesting story. Our cells are not passive victims of entropy—they are active maintenance systems, constantly repairing DNA, recycling damaged proteins, and policing their own quality control. Aging, in this view, is what happens when the rate of repair falls behind the rate of damage. The damage was always there. What changes with age is the cell’s willingness and ability to keep up.
The Fossel Framework: Intervene Upstream
Michael Fossel has spent decades making a pointed argument, most recently in Reversal: medicine keeps intervening downstream, treating symptoms one rung below the actual cause. He uses Alzheimer’s disease as his clearest example. First we tried drugs for the agitation and memory loss—pure symptom management. Then we targeted beta-amyloid plaques, which is one step closer to a cause. But, Fossel asks, what caused the amyloid to accumulate in the first place? We are still standing one step downstream of the real problem.
His proposed answer points to the cell itself. As a cell divides over a lifetime, the protective caps on the ends of its chromosomes—the telomeres—grow shorter. Fossel’s model holds that shortening telomeres act as a kind of dimmer switch on gene expression: as they erode, the cell throttles back its molecular repair and housekeeping. The cell doesn’t fail because damage is inevitable; it fails because its cleaning crews are told to slow down. Restore the signal—in the laboratory, by re-lengthening telomeres using the enzyme telomerase—and the cell can, remarkably, resume behaving like a younger cell.
“Aging is not inevitable.” The provocation at the heart of Fossel’s work is that if a single upstream mechanism drives many age-related diseases, then resetting that mechanism could address them as a class—rather than one expensive disease at a time.
Two honest caveats belong here. First, the most dramatic results—true age reversal in tissue—remain in the laboratory and in early-stage trials, not yet on the clinic shelf. Second, telomere biology is one powerful lens, not the whole picture; serious scientists debate how much of aging it explains. But as an organizing principle—find the upstream cause and reset it—Fossel’s framework is the right way to think about the next era of medicine. It is the intellectual spine of this paper.
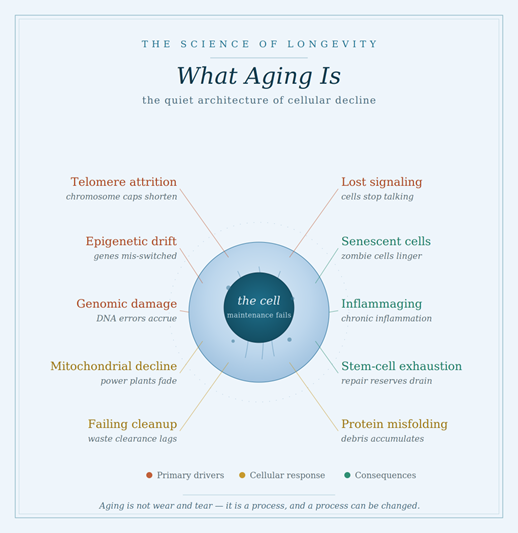
The Hallmarks of Aging: A Useful Map
Researchers commonly describe aging through a set of interlocking “hallmarks”—the measurable signs and mechanisms that accompany growing old. They are worth knowing because nearly every intervention in this paper targets one or more of them:
Telomere attrition — the shortening chromosome caps central to Fossel’s model.
Epigenetic alteration — changes in which genes are switched on or off, the basis of the aging “clocks” discussed below.
Mitochondrial dysfunction — the cell’s power plants producing less energy, a major focus of Greenfield’s work.
Cellular senescence — “zombie” cells that stop dividing but linger, leaking inflammatory signals.
Loss of proteostasis and impaired autophagy — the cell’s recycling and waste-clearance systems falling behind.
Chronic inflammation (“inflammaging”) and stem-cell exhaustion — the slow erosion of the body’s repair reserves.
Fossel’s contribution is to argue that these are largely symptoms and signs—invaluable for measurement, but not the root. The opportunity is to intervene above them.
Part II — What’s Possible Today: Measuring the Biological Clock
You cannot manage what you do not measure. The single most important shift of the past decade is that we can now estimate your biological age—how old your body actually behaves—independent of the candles on your birthday cake. Two people of the same chronological age can differ by fifteen or twenty biological years. Knowing your number, and watching it move, is the foundation of everything that follows.
Epigenetic Testing: The Aging “Clocks”
The most validated tools in this category are epigenetic clocks. They measure DNA methylation—small chemical tags that sit on your DNA and govern which genes are active. The pattern of these tags changes with age in a predictable enough way that algorithms (Horvath, GrimAge, DunedinPACE, and others) can estimate biological age and, in the case of pace-of-aging clocks, how fast you are aging right now.
For the individual, the value is not the single number—it is the trend. A methylation test repeated every six to twelve months turns lifestyle and therapy from a matter of faith into a measurable experiment. Did the new sleep routine, the strength training, the fasting protocol actually move the needle? The clock will tell you.
A Practical Testing Panel
Beyond the epigenetic clock, a thoughtful longevity work-up draws on widely available tests. The goal is to find risk a decade early, while you still have options—because, as I tell my patients, ignorance is a liability.
Epigenetic (DNA methylation) clock: Biological age and pace of aging; the master trend line.
hs-CRP and inflammatory markers: Hidden chronic inflammation—“inflammaging.”
Fasting insulin, HbA1c, glucose: Metabolic health and insulin resistance, often years before diabetes.
Advanced lipid panel (ApoB, Lp(a)): Cardiovascular risk with far more precision than standard cholesterol.
Comprehensive hormone panel: Thyroid, sex hormones, and cortisol rhythm across the day.
VO2 max and grip strength: Two of the strongest functional predictors of longevity.
DEXA / body composition: Muscle mass and visceral fat—mobility and metabolic destiny.
Advanced imaging (coronary calcium, MRI): Silent disease—early heart, cancer, or cognitive risk.
A panel like this reframes the annual physical. Instead of waiting for a symptom, you are running a risk assessment—exactly what any competent CEO does for the enterprise they are responsible for. Your body is that enterprise.
Part III — The Actionable Toolkit: Slowing the Clock Today
Here is the order of operations that matters, and where I depart from the gadget-first culture of much of the biohacking world. The foundation comes first. In Boundless, Ben Greenfield assembles an encyclopedic toolkit—but even he insists the advanced tools are multipliers, not substitutes. I say it this way: the turbochargers only work if the engine is running. Build the foundation first, then upgrade the hardware.
The principle that makes this toolkit coherent is the one that runs through this entire paper: every pathway of aging has a corresponding point of intervention. Before we walk through the tiers, the figure below maps each major pathway of decline to the kind of therapy that targets it.

Tier 1 — The Foundation (Free, Proven, Non-Negotiable)
No therapy in this paper can outrun a broken foundation. These are the highest-leverage longevity interventions known to science, and they cost nothing:
Nutrition: Real, whole, mostly unprocessed food. Adequate protein to defend muscle. Time-restricted eating or intermittent fasting to trigger autophagy—the cell’s self-cleaning process.
Movement: A combination of zone-2 cardiovascular work (to build the mitochondrial and aerobic base) and resistance training (to defend muscle mass, the single best functional predictor of a long, mobile life).
Sleep: Seven to eight hours, with sufficient deep sleep. Sleep is when the brain clears metabolic waste; chronic deprivation accelerates nearly every hallmark of aging.
Stress regulation: Meditation, breathwork, and nervous-system work. Chronic stress is a direct accelerant of biological aging.
Connection and purpose: The longest-lived populations on earth are not the most medicated—they are the most connected. Loneliness is a longevity risk factor on par with smoking.
Tier 2 — Intermediate Biohacks (Accessible, Evidence-Building)
Once the foundation is in place, a set of accessible interventions can act as genuine force multipliers. Many draw directly from Greenfield’s playbook and overlap with the light- and energy-based therapies I explore in my own clinical work:
Photobiomodulation (red and near-infrared light): Light at specific wavelengths is absorbed by the mitochondria, supporting cellular energy production. Investigated by NASA decades ago, it is now used for skin, recovery, inflammation, and increasingly cognition—with a near-zero risk profile for most people.
Heat and cold exposure: Sauna (especially infrared) and deliberate cold exposure trigger beneficial stress responses—improving cardiovascular resilience, mitochondrial function, and stress tolerance.
Exercise with Oxygen Therapy (EWOT): This is one of the most underused longevity tools in my clinical experience. The patient exercises while breathing concentrated oxygen, which floods the bloodstream—and especially the oxygen dissolved in plasma—far beyond what room air allows. The payoff is meaningful: improved oxygen delivery to tissues, enhanced mitochondrial energy production, reduced inflammation and lactic-acid load, and measurable gains in VO₂ max—one of the single strongest predictors of longevity we have. Because oxygen-transport efficiency naturally declines with age, EWOT is, in effect, a way to restore a more youthful delivery system while you train. I consider it a high-value addition to a serious longevity regimen.
Hyperbaric oxygen and breath work: Strategies to improve oxygen delivery and, in some protocols, signal tissue repair.
Targeted supplementation: Omega-3s, vitamin D, magnesium, and compounds that support cellular energy and methylation. Supplements fill gaps; they do not replace the foundation, and the supplement industry vastly overpromises—assess every claim with a skeptical, CEO’s eye.
Optimizing the “invisible” environment: Greenfield’s point that the air, water, light, and even the electrical environment of your home quietly shape your biology over decades is well taken—clean inputs compound.
Tier 3 — Advanced Interventions (Emerging, Clinician-Guided)
This tier sits at the frontier where today’s clinic meets tomorrow’s laboratory. These interventions are real and available in varying degrees, but they demand a qualified clinician, honest expectations, and respect for what is established versus what is still experimental:
Peptide therapies: Short chains of amino acids that signal specific repair and metabolic processes; a fast-evolving area requiring medical supervision and attention to regulatory status.
Senolytics: Compounds being studied for their ability to clear senescent “zombie” cells, with promising animal data and early human investigation.
NAD+ restoration: Approaches aimed at replenishing a coenzyme central to cellular energy and DNA repair that declines with age.
The horizon—telomerase and cellular reprogramming: Fossel’s gene-therapy approach and the broader field of partial cellular reprogramming aim to reset the cell’s age directly. This is where “reversal” stops being a metaphor—and it is the subject of the final section.
One category deserves far more than a bullet point—and it is the area where I have the deepest personal clinical experience. Regenerative medicine has earned its own section, which follows.
A rule for the frontier: the more controversial the therapy, the greater the obligation to understand the mechanism and the evidence before you reach for it. Boldness and rigor are not opposites.
Part IV — Regenerative Medicine: Healing From the Inside Out
If the rest of this paper is about slowing the clock, regenerative medicine is about something more ambitious—helping the body repair and rebuild tissue it would otherwise surrender to age and injury. As a spine surgeon, I have spent my career at the receiving end of degeneration: the worn discs, the failing joints, the tissue that simply stops healing the way it once did. Regenerative medicine is the most direct attempt yet to intervene in that process, and it maps cleanly onto Fossel’s principle—address the cause, not just the symptom.
The field works largely through paracrine signaling—the language cells use to instruct one another. Rather than surgically replacing a part, the goal is to deliver the right biological signals to the right location and let the patient’s own cells do the repair. The therapies below sit on a spectrum from the well-established to the genuinely cutting-edge.
Autologous Therapies (From Your Own Body)
Autologous means the material comes from you—which keeps the risk profile favorable and sidesteps many regulatory and ethical questions. These are the most widely available regenerative options in the United States today:
Platelet-Rich Plasma (PRP): Your own blood is concentrated to multiply its platelets, which carry a payload of growth factors. Injected at a precise site of injury—a tendon, a joint, a ligament—PRP delivers a concentrated burst of the body’s native healing signals. It is one of the most established regenerative tools, and patient selection and accurate targeting of the true pain generator matter enormously to the outcome.
Autologous stem-cell and bone-marrow / adipose-derived therapies: Cells harvested from your own bone marrow or fat tissue, then concentrated and reintroduced to support repair. Used widely in orthopedic and regenerative contexts, these remain an area of active research and require careful, evidence-guided clinical judgment.
Exogenous Stem Cells (From a Donor Source)
Beyond autologous approaches lies a category of donor-derived (“exogenous”) cellular therapies—often using cells from birth tissues such as umbilical cord or placental sources, which are rich in young, biologically active cells. These therapies are far more common in international clinics than in the United States, where the regulatory framework is more restrictive. Patients increasingly travel abroad for them, and it is important to be clear-eyed about this reality: the science is promising, the quality control across clinics is highly variable, and a thoughtful patient asks hard questions about sourcing, processing, evidence, and informed consent before pursuing treatment overseas. I include this category not as an endorsement of medical tourism, but because an honest map of the field has to acknowledge where the world is actually going.
The Next Generation: The Regenerative Protein Array (RPA)
The most exciting development I have encountered in this space moves beyond delivering cells—and focuses instead on delivering the full library of signals that orchestrate healing. The leading example is the Regenerative Protein Array (RPA) developed by Genesis Regenerative.
Where PRP delivers a concentrated but relatively narrow set of growth factors, RPA is a sophisticated, placental-tissue–derived array containing more than 80 distinct cytokines, growth factors, and microRNA (miRNA). It is best understood as a generation beyond PRP and exosomes. Rather than supplying raw material, it supplies instructions—a complex cocktail of bioactive molecules that, through paracrine signaling, effectively help “reprogram” the local environment of damaged tissue and activate the patient’s own innate healing machinery. In other words, it speaks to the cell in the cell’s own language, and on a far broader bandwidth than earlier tools.
This breadth is the point. Healing is never the work of a single molecule; it is an orchestrated sequence—reducing inflammation, recruiting cells, building new blood supply, laying down matrix. A therapy that can present the body with the full ensemble of signals, rather than a single instrument, is conceptually aligned with everything this paper argues: intervene upstream, at the level of cellular communication, and let the body’s own intelligence do the rest. RPA has been applied across a range of physical, cognitive, and anti-aging applications by clinicians in multiple specialties.
For readers who want to go deeper into the science, mechanism, and clinical applications of the Regenerative Protein Array, Genesis Regenerative maintains detailed educational resources at genesisregenerative.com.
As with everything at the frontier, the right posture is informed enthusiasm: real promise, paired with the discipline to ask for mechanism, evidence, transparency, and proper informed consent. These statements have not been evaluated by the FDA, and regenerative therapies should be pursued only in partnership with a qualified clinician.
Part V — Where We Are Going: The Next Decade
If Part I described a new understanding and Parts II–III described what you can do this year, this section is about the trajectory—the reason I believe we are living through an inflection point rather than an incremental improvement.
From managing disease to resetting the cell. The Fossel thesis—intervene upstream, reset cellular function rather than chase symptoms—is moving from theory toward trials. Telomerase gene therapy aimed at age-related disease is being actively developed. Even partial success would reframe how we treat Alzheimer’s, cardiovascular disease, and frailty as a connected class.
From small molecules to biological information. Medicine is shifting from pills toward gene therapy, mRNA, and cellular reprogramming—delivering instructions to cells rather than blunt chemicals. This is a different kind of medicine, aimed at causes rather than consequences.
From population averages to the individual. AI and continuous biomarkers—wearables, frequent epigenetic testing, real-time data—will make longevity care personalized and dynamic, adjusting in months rather than decades.
From sick-care to health-span. The economic and human case is overwhelming: it is far cheaper, and infinitely more humane, to compress decline into the final months of a long life than to fund decades of managed deterioration.
None of this erases honest uncertainty. Timelines in this field have a long history of optimism outpacing data, and a responsible physician says so plainly. But the direction is unmistakable, and the foundational actions in Part III lose you nothing while the frontier matures. You position yourself to benefit from tomorrow’s breakthroughs by protecting your biology today.
Conclusion: Become the CEO of Your Own Longevity
The throughline of this paper, and of my life’s work, is a transfer of ownership. For a century, you were a passenger—handed a diagnosis, handed a prescription, told that aging was simply what happened next. The science described here hands you the wheel.
Fossel gives us the principle: aging is a process with a cause, and causes can be addressed. Greenfield gives us the practice: an honest, foundation-first toolkit anyone can begin today. My contribution, as a surgeon who has seen too many lives narrowed by preventable decline, is to insist on the right order of operations—foundation first, measurement always, frontier with eyes open.
We are not waiting for permission from a broken system. The tools to measure your biological age, slow your decline, and prepare for the coming era of cellular medicine exist now. The question is no longer whether longevity science is real. The question is whether you will act on it.
Start by measuring. Build the foundation. Add the multipliers. Watch your numbers move. And stay close to the frontier—because it is arriving at the speed of light.
A Note on Sources & Disclaimers
This white paper is intended for educational purposes and synthesizes ideas from two foundational works the reader is encouraged to explore directly: Reversal: Science, Medicine, and a Future Beyond Aging by Michael Fossel, M.D., Ph.D., and Boundless by Ben Greenfield. The interpretations, framing, ordering, and clinical opinions are my own.
Nothing here constitutes individualized medical advice. The advanced and regenerative interventions discussed range from well-established to genuinely experimental; several require a qualified physician, and regulatory status varies. Before beginning any testing protocol, supplement, or therapy, consult a clinician who knows your history. The goal of this paper is not to hand you answers—it is to make you a more informed, more empowered participant in your own longevity.
Selected References
Fossel, M. (2026). Reversal: Science, Medicine, and a Future Beyond Aging. Independently published.
Greenfield, B. (2020). Boundless: Upgrade Your Brain, Optimize Your Body & Defy Aging. Victory Belt Publishing.
López-Otín, C., Blasco, M. A., Partridge, L., Serrano, M., & Kroemer, G. (2013). The hallmarks of aging. Cell, 153(6), 1194–1217.
López-Otín, C., Blasco, M. A., Partridge, L., Serrano, M., & Kroemer, G. (2023). Hallmarks of aging: An expanding universe. Cell, 186(2), 243–278.
Horvath, S. (2013). DNA methylation age of human tissues and cell types. Genome Biology, 14(10), R115.
Belsky, D. W., Caspi, A., Corcoran, D. L., et al. (2022). DunedinPACE, a DNA methylation biomarker of the pace of aging. eLife, 11, e73420.