
Migraine Remission Protocols
Break the Loop. Ground the Lightning. Calm the Storm.
A migraine is not "just a headache." It is a neurological electrical storm caused by a mitochondrial energy crisis. We use advanced biophysics to stabilize the grid.
Accolades

Ready to Get Started?
Fill out the form to request an appointment at our Edina clinic. We're here to answer your questions and guide you on your journey to better health. We Accept HSA, FSA, Worker's Compensation, Care Credit, In-house financing.
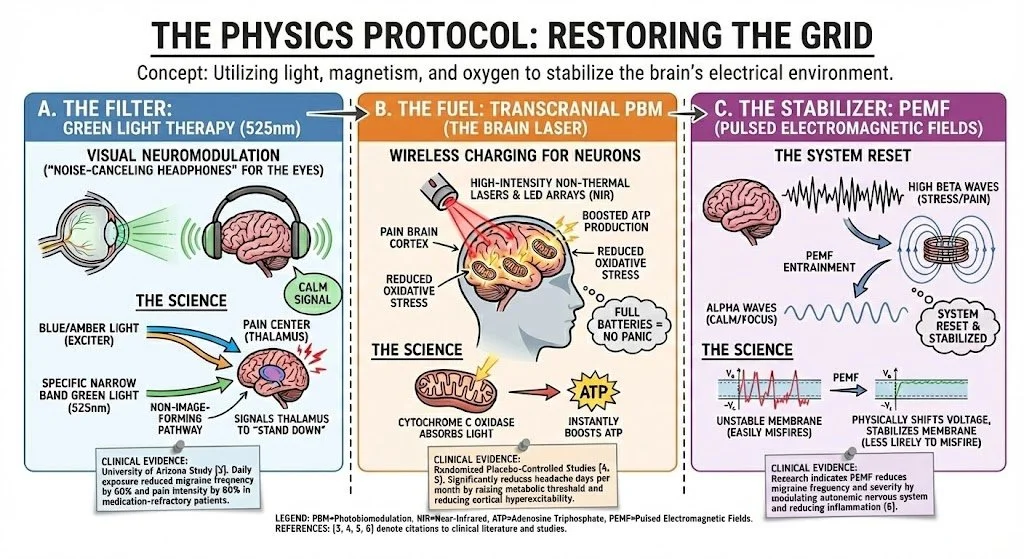
THE PHYSICS PROTOCOL: RESTORING THE GRID
We use light, magnetism, and oxygen to stabilize the brain's electrical environment.
A. THE FILTER: GREEN LIGHT THERAPY (525nm)
The Concept: Visual Neuromodulation. Think of this as "noise-canceling headphones" for your eyes.
The Science: Unlike blue or amber light, which excites the retina and triggers the thalamus (pain center), a specific narrow band of Green Light (525nm) generates significantly smaller electrical signals. It travels a unique non-image-forming pathway from the eye to the brain, signaling the thalamus to "Stand Down" [3].
The Evidence: A breakthrough University of Arizona study found that daily exposure to specific green light reduced migraine frequency by 60% and pain intensity by 60% in patients who had failed standard medication [3].
B. THE FUEL: TRANSCRANIAL PBM (The Brain Laser)
The Concept: Wireless Charging for Neurons.
The Science: We use high-intensity, non-thermal Class IV Lasers and LED arrays to deliver Near-Infrared (NIR) light through the skull directly to the cortex. This light is absorbed by Cytochrome C Oxidase in the mitochondria, instantly boosting ATP production and reducing oxidative stress [4]. A brain with full batteries doesn't panic.
The Evidence: Randomized placebo-controlled studies demonstrate that Transcranial PBM significantly reduces the number of headache days per month by raising the brain's metabolic threshold and reducing cortical hyperexcitability [5].
C. THE STABILIZER: PEMF (Pulsed Electromagnetic Fields)
The Concept: The System Reset.
The Science: Migraine brains often get stuck in "High Beta" waves (Stress/Pain). We use PEMF to entrain the brain down to "Alpha" (Calm/Focus). It physically shifts the voltage of the cell membrane, making neurons less likely to misfire.
The Evidence: Research indicates that PEMF therapy can reduce the frequency and severity of migraine attacks by modulating the autonomic nervous system and reducing inflammation [6].
A MESSAGE TO THE PATIENT: WE KNOW THE COST
We Know the Cost: If you are reading this, you know that "headache" is an insult to what you experience. A migraine is a thief. It steals your days, your focus, and your joy. It is the missed birthdays, the canceled meetings, and the constant, low-level anxiety that a storm is brewing behind your eyes. It is the "migraine hangover" (postdrome) that leaves you feeling like a ghost in your own life even after the pain stops.
The Standard Failure: You have likely climbed the "Pill Ladder"—from Excedrin to Triptans, to Topamax, and now the monthly CGRP injections. While these tools can help survive a crash, they act as chemical fire extinguishers. They do not repair the wiring. They often come with a heavy tax: brain fog, fatigue, and the dreaded "rebound cycle" (Medication Overuse Headache).
The HyperCharge Shift: We do not view Migraine as a disease of pain; we view it as a failure of energy management. Your brain is a high-performance engine running too hot, with a cooling system that has failed. We don't just numb the nerves. We engineer remission by increasing your brain's voltage (fuel) and decreasing its excitability (noise).
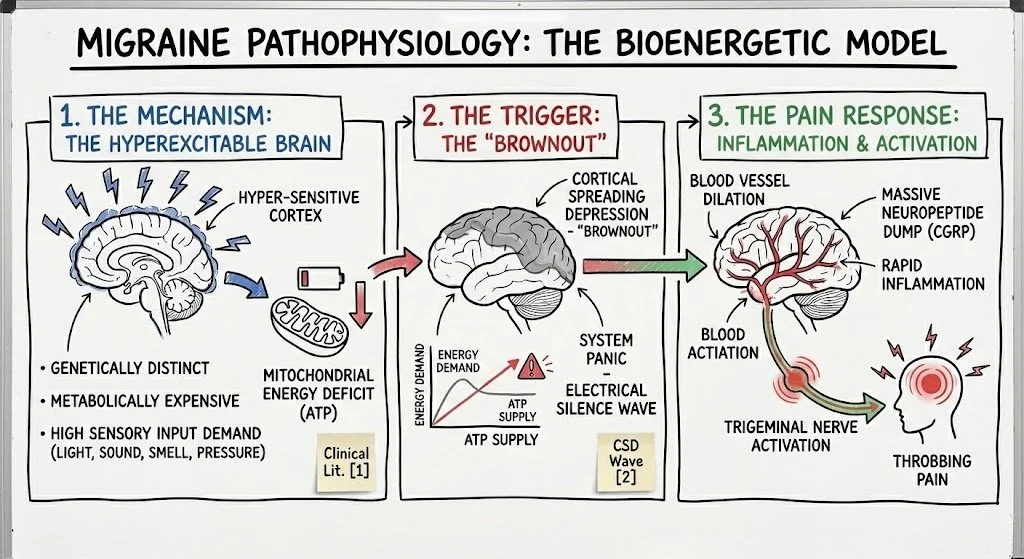
THE SCIENCE OF HOPE: THE "ENERGY CRISIS"
To treat migraine effectively, you must understand the physics of why it happens.
The Mechanism: The Hyperexcitable Brain The migraine brain is genetically distinct. It is "metabolically expensive." It burns through energy faster than the average brain because it is hyper-sensitive to sensory input (light, sound, smell, barometric pressure). This deficit in mitochondrial energy reserve is well-documented in clinical literature [1].
The Trigger: The "Brownout" When your brain's demand for energy outstrips its supply of ATP (cellular fuel), the system panics. It initiates a wave of electrical silence called Cortical Spreading Depression (CSD). This is the "brownout" [2]. In response, the brain dumps a massive load of inflammatory neuropeptides (CGRP) to dilate blood vessels and flush the system. This rapid inflammation irritates the Trigeminal Nerve. That is the throbbing pain you feel.
Our Solution: We stop the brownout. We use Photobiomodulation to supercharge your mitochondria (batteries) so they can handle the load, and Neuromodulation to calm the sensors so they stop pulling the fire alarm.

THE BIOCHEMICAL PROTOCOL: SIGNALING REPAIR
We treat the chemical "wildfire" with targeted signaling molecules.
-
Important Medical Disclosure: Peptides are prescribed off-label. They are not FDA-approved for the treatment of Migraine. Their use is based on global research and clinical experience as part of a comprehensive protocol.
BPC-157: Known as the "Body Protection Compound," this peptide is used to dampen systemic neuro-inflammation and repair the Gut-Brain Axis. Dysbiosis and "leaky gut" are heavily correlated with migraine frequency [7].
Thymosin Alpha-1: A master immune modulator used to calm the "Cytokine Storm" (specifically TNF-alpha and IL-6) that often precedes or accompanies a migraine attack [8].
-
Magnesium Threonate: The only form of magnesium that effectively crosses the Blood-Brain Barrier. Studies show magnesium deficiency plays a key role in CSD and migraine pathogenesis [9].
Riboflavin (B2) & CoQ10: The "Mitochondrial Cocktail." These are the essential spark plugs for ATP production. High-dose Riboflavin is a Class B recommendation by the American Academy of Neurology for migraine prophylaxis [10].
THE NEUROMODULATION PROTOCOL: EXOMIND TMS
FDA-Cleared technology to stop the storm.
The Tech: ExoMind Transcranial Magnetic Stimulation (TMS). The Mechanism:
Stopping the Wave: Migraines are driven by an electrical wave (Cortical Spreading Depression). TMS delivers a precise magnetic pulse that disrupts this wave, effectively hitting the "Reset Button" on the brain's electrical activity.
Treating the Anxiety Loop: Chronic migraine creates "Anticipatory Anxiety"—the constant fear of the next attack. TMS treats the anxiety centers of the brain directly, breaking the stress-pain loop. The Evidence: A landmark study in The Lancet Neurology demonstrated that single-pulse TMS was effective for the acute treatment of migraine with aura, with 39% of patients pain-free at 2 hours [11].
REALITY CHECK
What We Aim To Do:
Reduce Frequency: Turn chronic migraine (15+ days/month) into manageable episodic migraine (<4 days/month).
Reduce Severity: Make attacks manageable with over-the-counter meds, keeping you out of the ER.
Engineer Remission: Give you your life back.
What We Cannot Do:
We do not promise a "Cure." Migraine is a genetic neurological architecture. Our goal is high-performance management and remission.
We do not treat "Thunderclap Headaches" (sudden, worst headache of life)—this is a medical emergency requiring the ER.
Frequently Asked Questions
-
No. This is the paradox. Green light is uniquely soothing. Most patients feel an immediate physical "sigh of relief" in their brain when the green light turns on.
-
Yes. Our therapies are safe to combine with your current medications. By lowering the inflammatory load, we often make those medications work better or help you taper off them over time.
-
HyperCharge operates on a direct-care model. This allows us to use advanced technologies (Class IV Laser, Neuro20, ExoMind) that insurance companies are typically 10-15 years behind in covering.
Stop Managing the Crash. Start Preventing It.
You do not have to live your life in a dark room. You do not have to cancel another birthday party. Your brain is not broken; it is just starving for energy and overwhelmed by noise. Biology is listening. It is waiting for the right signal to calm the storm.
HyperCharge is Hope. Come to the Lab. Let us audit your triggers, check your brain's voltage, and build a protocol to break the loop.
SCIENTIFIC REFERENCES
Lodi, R., et al. (2001). "Energy metabolism in migraine patients: a 31P-MRS study." Brain, 124(11), 2229-2236. [Demonstrates mitochondrial deficit in migraineurs].
Pietrobon, D., & Moskowitz, M. A. (2013). "Pathophysiology of migraine." Annual Review of Physiology, 75, 365-391. [Establishes Cortical Spreading Depression mechanism].
Martin, L.F., et al. (2021). "Green Light Exposure Improves Pain and Quality of Life in Fibromyalgia and Migraine Patients." Cephalalgia, 41(2), 135-147.
Hamblin, M. R. (2016). "Photobiomodulation: the mechanism of action." BME Frontiers, 2016, 1-15.
Kindler, S., et al. (2019). "Transcranial Photobiomodulation in the Management of Chronic Migraine: A Review of Mechanisms." The Journal of Headache and Pain, 20(1), 1-12.
Thomas, A. W., et al. (2007). "A randomized, double-blind, placebo-controlled clinical trial using a low-frequency magnetic field in the treatment of musculoskeletal chronic pain." Pain Research & Management, 12(4), 249-258.
Arzani, M., et al. (2020). "Gut-brain Axis and migraine headache: a comprehensive review." The Journal of Headache and Pain, 21(1), 1-12.
Yucel, M., et al. (2016). "Increased levels of oxidative stress markers and proinflammatory cytokines in migraine patients." Cellular and Molecular Biology, 62(1), 1-5.
Dolati, S., et al. (2020). "The Role of Magnesium in Pathophysiology and Migraine Treatment." Biological Trace Element Research, 196(2), 375-383.
Holland, S., et al. (2012). "Evidence-based guideline update: NSAIDs and other complementary treatments for episodic migraine prevention in adults." Neurology, 78(17), 1346-1353.
Lipton, R.B., et al. (2010). "Single-pulse transcranial magnetic stimulation for acute treatment of migraine with aura: a randomised, double-blind, parallel-group, sham-controlled trial." The Lancet Neurology, 9(4), 373-380.