
Trigeminal Neuralgia Treatment
Cooling the Fire. Insulating the Wire. Healing the Shock.
You live in fear of the next shock. Standard medicine offers sedation or brain surgery. We offer non-invasive engineering to help repair the short circuit.
Accolades

Ready to Get Started?
Fill out the form to request an appointment at our Edina clinic. We're here to answer your questions and guide you on your journey to better health. We Accept HSA, FSA, Worker's Compensation, Care Credit, In-house financing.
THE PHYSICS PROTOCOL: NON-INVASIVE DECOMPRESSION
We use high-energy physics to calm the nerve and reduce the pressure.
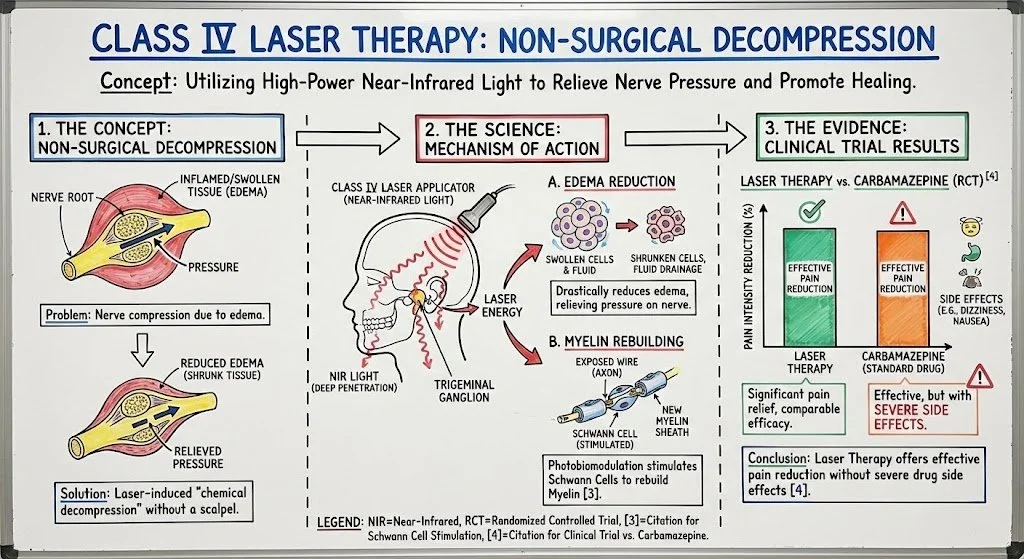
A. THE HEALER: CLASS IV LASER THERAPY
The Concept: Non-Surgical Decompression.
The Science: We use high-power Near-Infrared light applied externally to the jaw, neck, and mastoid process to penetrate deep to the Trigeminal ganglion. Laser energy is proven to drastically reduce edema (swelling). By shrinking the inflamed tissue around the nerve root, we relieve the pressure—effectively performing a "chemical decompression" without a scalpel. Furthermore, Photobiomodulation stimulates Schwann Cells, which are responsible for rebuilding the Myelin sheath [3].
The Evidence: A pivotal randomized controlled trial compared Laser Therapy directly against Carbamazepine (the standard drug). The study found that Laser Therapy was effective in reducing pain intensity without the severe side effects of the medication [4].
B. THE FILTER: GREEN LIGHT THERAPY
The Concept: Calming the "Pain Brain."
The Science: TN creates a "Pain Loop" in the thalamus. Even when the shock isn't happening, the brain is hyper-vigilant, waiting for it. Specific wavelengths of green light (525nm) activate a unique pathway that sedates the thalamus, lowering background anxiety and raising the pain threshold [5].
C. THE SYSTEM RESET: PEMF (Pulsed Electromagnetic Fields)
The Concept: The Voltage Regulator.
The Science: TN puts your body in a state of extreme Sympathetic Stress (Fight or Flight). We use PEMF to shift your nervous system from "Panic" to "Repair." It reduces the excitability of C-fibers (pain nerves), making them less likely to fire randomly.
The Evidence: Studies demonstrate that PEMF treatment significantly reduces neuropathic pain levels and oxidative stress markers, suggesting a direct protective effect on nerve tissue [6].
A MESSAGE TO THE PATIENT: WE KNOW THE Fear
We Know the Cost: If you are reading this, you are living in a state of constant, low-grade terror. Trigeminal Neuralgia (TN) is called "The Suicide Disease" for a reason. It is widely considered the most excruciating pain a human being can experience. You know the feeling of a 10,000-volt shock hitting your face just because a breeze touched your cheek or you brushed your teeth. You are afraid to eat. You are afraid to speak. You are afraid to smile.
The Standard Failure: You have likely been put on heavy anti-seizure medications like Carbamazepine (Tegretol) or Gabapentin. These drugs act as a chemical blanket, smothering your brain's electrical activity. They often turn you into a "zombie," forcing you to choose between excruciating pain and cognitive function. Or, you are facing the prospect of Microvascular Decompression (MVD)—invasive brain surgery with significant risks.
The HyperCharge Shift: We reject the binary choice between "Sedation" and "Surgery." We view TN as a problem of Bio-Electric Instability. The nerve is misfiring because it has lost its insulation (Myelin) and is inflamed. We use Human Engineering—specifically Class IV Laser and Neural Calming protocols—to reduce that inflammation and stimulate the nerve to heal itself, without cutting into your skull or dulling your mind.
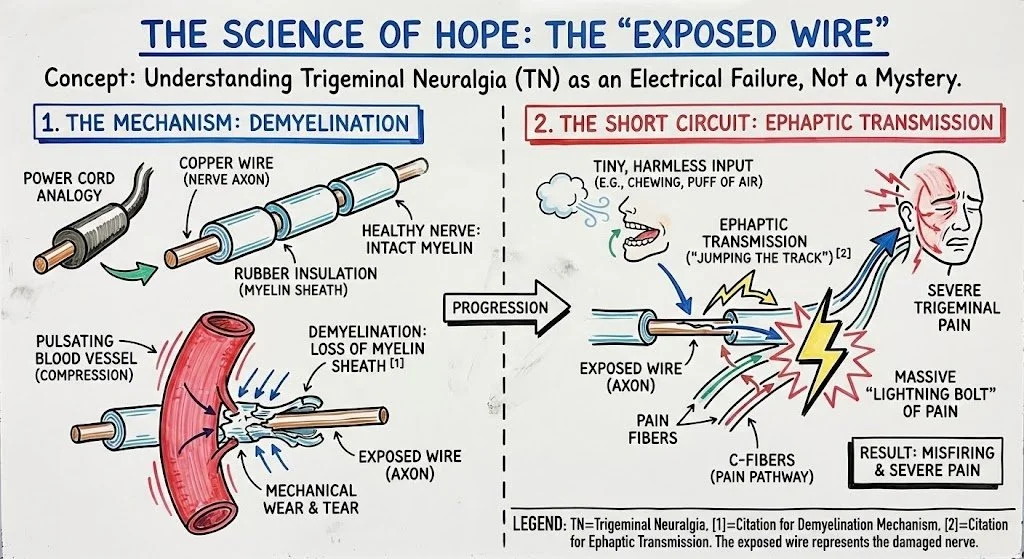
THE SCIENCE OF HOPE: THE "Exposed Wire"
To treat TN effectively, you must understand it as an electrical failure, not a mystery.
The Mechanism: Demyelination Imagine a power cord. Inside is the copper wire (the nerve axon), and outside is the rubber insulation (the Myelin Sheath). In Trigeminal Neuralgia, a blood vessel often pulsates against the nerve root, mechanically wearing away the insulation. This process is called demyelination [1].
The Short Circuit: Ephaptic Transmission Now, you have an exposed wire. A tiny, harmless input—like chewing or a puff of air—hits that exposed wire and "jumps the track" to the pain fibers. This triggers a massive "Lightning Bolt" of pain. This cross-talk is known as Ephaptic Transmission [2].
Our Solution: We cannot move the vessel without surgery. But we CAN reduce the swelling (creating space) and stimulate the Schwann Cells to repair the insulation (Myelin) using Physics.

THE BIOCHEMICAL PROTOCOL: SIGNALING REPAIR
We treat the nerves with targeted molecules to support re-insulation.
-
Important Medical Disclosure: Peptides are prescribed off-label. They are not FDA-approved for the treatment of TN. Their use is based on global research and clinical experience.
ARA-290 (Cibinetide): This is critical. ARA-290 is specifically studied for Small Fiber Neuropathy and nerve repair. It targets the "innate repair receptor" (IRR) to turn off pain signals and promote nerve healing and myelination [7].
BPC-157: A systemic peptide used to reduce neuro-inflammation and protect nerve integrity.
-
Methyl-B12 (High Dose Injections): Vitamin B12 is the raw material of Myelin. Oral supplements are often not absorbed well enough to repair damage. We optimize levels to support re-insulation [8].
Magnesium Threonate: The only form of magnesium that crosses the blood-brain barrier effectively to calm nerve excitability.
Omega-3 Fatty Acids: Used to dampen the systemic inflammation driving the pressure.
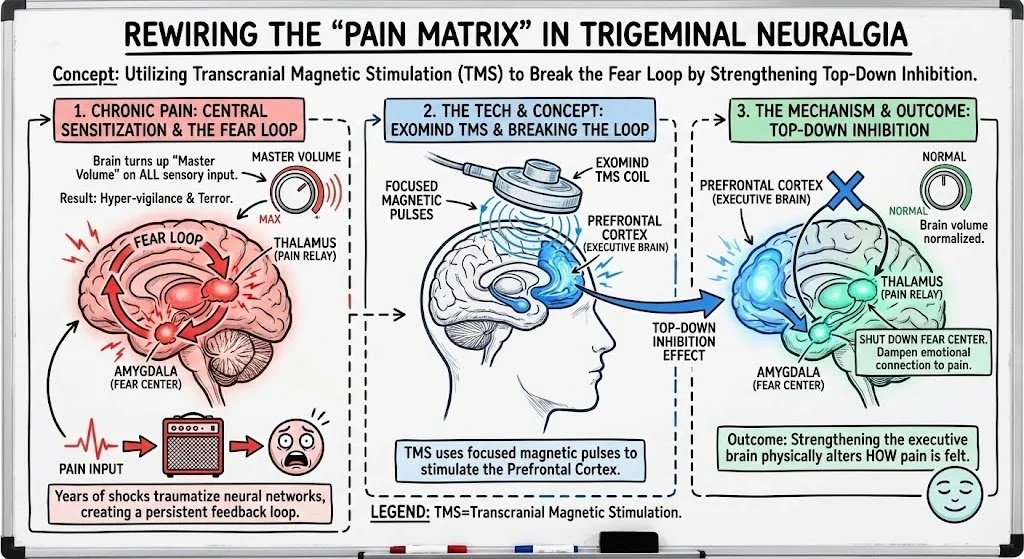
THE MENTAL HEALTH PROTOCOL: REWIRING THE "PAIN MATRIX"
TN is not just a nerve problem; it is a brain problem. Years of shocks have traumatized your neural networks. We treat the central processing unit that interprets the pain.
The Tech: ExoMind Transcranial Magnetic Stimulation (TMS).
The Concept: Breaking the Fear Loop.
The Science: Chronic pain causes Central Sensitization. Essentially, your brain turns up the "Master Volume" on all sensory input, making you hyper-vigilant and terrified. This creates a feedback loop between the Thalamus (pain relay) and the Amygdala (fear center). TMS uses focused magnetic pulses to stimulate the Prefrontal Cortex. This creates a "Top-Down" inhibition effect—it strengthens the executive brain so it can tell the fear center to shut down. By dampening the emotional connection to the pain, we physically alter how the pain is felt.
The Evidence: A systematic review in The Journal of Pain confirmed that high-frequency rTMS of the motor cortex significantly reduces pain intensity in refractory neuropathic pain conditions, including Trigeminal Neuralgia, by modulating the brain's opioid system [9]. Furthermore, treating the comorbid depression/anxiety with FDA-Cleared protocols creates a "physiological lift" that raises the patient's pain tolerance threshold [10].
REALITY CHECK
What We Aim To Do:
Remission: Reduce the frequency and intensity of shocks so you can eat, speak, and live without fear.
Medication Reduction: Help you lower the dose of Tegretol or Gabapentin (under your doctor's supervision) to clear the "brain fog."
Avoid Surgery: Delay or prevent the need for Microvascular Decompression.
What We Cannot Do:
We cannot "move" a blood vessel that is physically compressing the nerve (only surgery does that). However, by reducing inflammation, we often relieve the pressure enough to stop the pain.
We cannot treat active cancer in the facial/neck region with Laser.
Frequently Asked Questions
-
No. The laser uses light, not vibration or electricity. It is non-contact and creates a gentle, soothing warmth. Most patients find it immediately relieving.
-
No. Stopping Tegretol suddenly can be dangerous. Our goal is to reduce your pain naturally so that your prescribing doctor can gradually taper your medication over time.
-
No. Gamma Knife is radiation that intentionally damages the nerve to stop the signal. Our Laser Therapy is Regenerative—it heals the nerve to stop the signal. It is non-destructive.
You Don't Have to Live in Fear.
The "shock" is a sign of a nerve in crisis. It is crying out for energy and repair, not just sedation. You have options between "Drugs" and "Brain Surgery." It is called Engineering. Do not accept a life of fear. Do not accept the "Zombie" state.
HyperCharge is Hope. Come to the Lab. Let us audit your inflammation, check your nerve health, and build a protocol to cool the fire.
SCIENTIFIC REFERENCES
Love, S., & Coakham, H. B. (2001). "Trigeminal neuralgia: pathology and pathogenesis." Brain, 124(12), 2347-2360.
Devor, M., et al. (2002). "Pathophysiology of Trigeminal Neuralgia: The Ignite Hypothesis." The Clinical Journal of Pain, 18(1), 4-13.
Chow, R., et al. (2011). "Inhibitory Effects of Laser Irradiation on Peripheral Mammalian Nerves and Relevance to Analgesic Effects: A Systematic Review." Lasers in Medical Science, 26(6), 833-842.
Ebrahimi, H., et al. (2018). "Laser Therapy versus Tegretol in Trigeminal Neuralgia: A Randomized Double-Blind Controlled Trial." Journal of Lasers in Medical Science, 9(3), 186-190.
Martin, L.F., et al. (2021). "Green Light Exposure Improves Pain and Quality of Life in Fibromyalgia and Migraine Patients." Cephalalgia, 41(2), 135-147.
Mert, T., et al. (2017). "Pulsed Magnetic Field Treatment Reduces Neuropathic Pain Symptoms and Spinal Oxidative Stress." Bioelectromagnetics, 38(1), 48-58.
Brines, M., et al. (2014). "ARA 290, a nonerythropoietic peptide engineered from erythropoietin, improves metabolic control and neuropathic pain in patients with type 2 diabetes." Molecular Medicine, 20, 658-666.
Zhang, M., et al. (2013). "Methylcobalamin: a potential vitamin of pain killer." Neural Plasticity, 2013, 424651.
Galhardoni, R., et al. (2019). "Repetitive Transcranial Magnetic Stimulation in Chronic Pain: A Review of the Literature." Archives of Physical Medicine and Rehabilitation, 100(8), 1547-1559.
Leung, A., et al. (2009). "rTMS for Suppressing Neuropathic Pain: A Meta-Analysis." The Journal of Pain, 10(12), 1205-1216.