
The Crumbling Frame: Why We Are Losing the War on Osteoporosis (And How Engineering Can Win It)
By Dr. Stefano Sinicropi - Founder, The HyperCharge Health Human Engineering Lab, Echolight Scientific Advisory Board, Board Certified Orthopedic Spine Surgeon
Disclaimer: This blog is for informational purposes only and does not constitute medical advice. The content is not intended to be a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
THE PREMISE: A PARADOX OF FAILURE
If you analyze the trajectory of osteoporosis management over the last two decades, you find a disturbing paradox. The prescription of anti-resorptive medications (Bisphosphonates) has been widespread since the 1990s. We have more drugs, more screening awareness, and more "calcium chews" on the market than ever before.
Yet, the burden of fragility fractures remains catastrophic. The statistics are not just numbers; they are a condemnation of our current approach:
The Mortality Crisis: The one-year mortality rate following a hip fracture is between 20% and 30% [1]. That is a higher death rate than many cancers.
The Morbidity Crisis: Of those who survive, 50% never regain their previous level of mobility [2].
The Future Crisis: The International Osteoporosis Foundation estimates that by 2050, the worldwide incidence of hip fractures will increase by 310% in men and 240% in women [3].
Why are we failing? Because standard medicine is treating a Physics and Lifestyle problem with a Chemical solution. We are attempting to chemically harden the bone without addressing the structural, hormonal, and metabolic failures that caused the frame to crumble in the first place.
THE SURGEON’S PERSPECTIVE: OPERATING ON CHALK
As a spine surgeon, I do not just read about bone density; I feel it. I face the "Surgical Cliff" that standard care ignores.
When I perform a fusion on a patient with severe osteoporosis, I am effectively trying to weld steel screws into wet drywall.
Instrumentation Failure: Osteoporosis drastically reduces "screw pullout strength." Studies show that patients with poor bone quality have a significantly higher rate of screw loosening, cage subsidence, and proximal junctional kyphosis (PJK) [4].
The Vicious Cycle: If the bone is too weak to hold the hardware, the surgery fails. We have to re-operate. But re-operating on broken bone leads to diminishing returns and exponentially higher risks.
We cannot simply "hardware" our way out of a biological failure. We must engineer the bone before the fracture occurs.
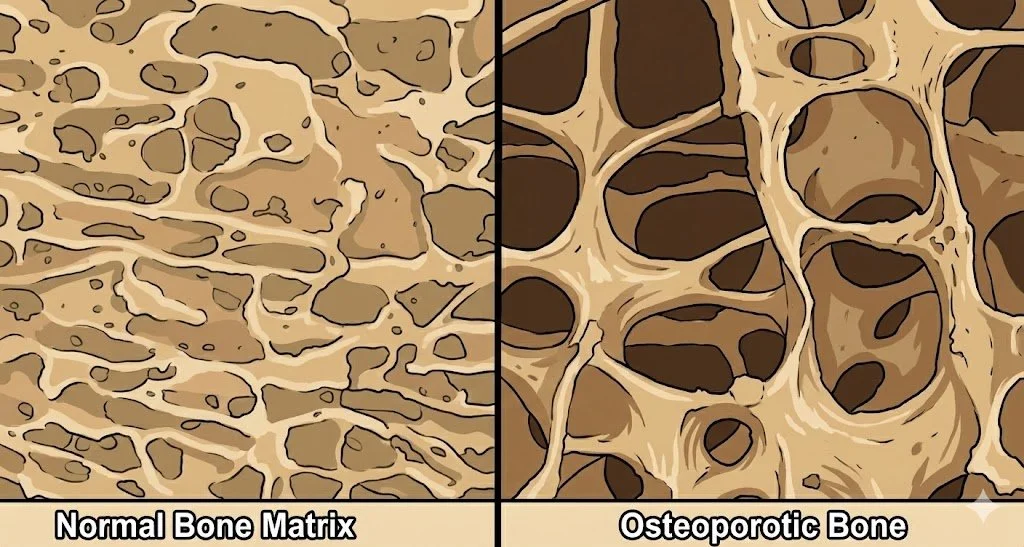
THE "DEAD ROCK" FALLACY
Standard medicine treats bone like a static mineral deposit. Bone is not a rock. It is a living, piezoelectric crystal.
It obeys Wolff’s Law (1892), which dictates that bone remodeling is driven by mechanical load [5]. When bone is stressed, it generates an electrical charge (Piezoelectricity) that attracts calcium ions. If you simply coat the bone in medication without restoring the mechanical load (Muscle/Gravity) and the electrical environment (Voltage), you are painting over a rusted bridge.
THE MEDICATION TRAP: A CRITICAL ANALYSIS
I am not anti-medication. Powerful anabolic agents like Forteo (Teriparatide) and Tymlos (Abaloparatide) are essential tools for rebuilding bone mass in severe cases.
However, the over-reliance on Bisphosphonates (e.g., Fosamax) as a first-line prevention strategy for osteopenia warrants scrutiny.
Mechanism: These drugs inhibit osteoclasts (the cells that recycle old bone).
The Consequence: While bone density (BMD) may increase, the natural remodeling cycle is frozen. Old, micro-damaged bone is not cleared away. This can lead to "frozen bone" that is dense but brittle.
The Risk Profile: Long-term suppression of bone turnover has been linked to Osteonecrosis of the Jaw (ONJ) [6] and Atypical Femoral Fractures—breaks that occur spontaneously because the bone has lost its elasticity [7].
We must ask: Is freezing the bone the best way to save it? Or should we focus on stimulating the Osteoblasts (builders) to construct new frame?
THE HYPERCHARGE PROTOCOL: A 5-PILLAR ENGINEERING APPROACH
Under my direct supervision at The HyperCharge Human Engineering Lab, we employ a multimodal strategy to restore bone quality, not just density.
THE HORMONAL FOUNDATION
Bone is hormone-dependent tissue. You cannot build a skyscraper without a project manager.
Testosterone (Men): It is not just for libido. The ResTOS Study showed that testosterone treatment significantly increased volumetric bone density and strength in older men [8].
Estrogen (Women): The decline of estrogen is the primary driver of post-menopausal resorption. Bio-identical optimization is often the most direct "root cause" fix.
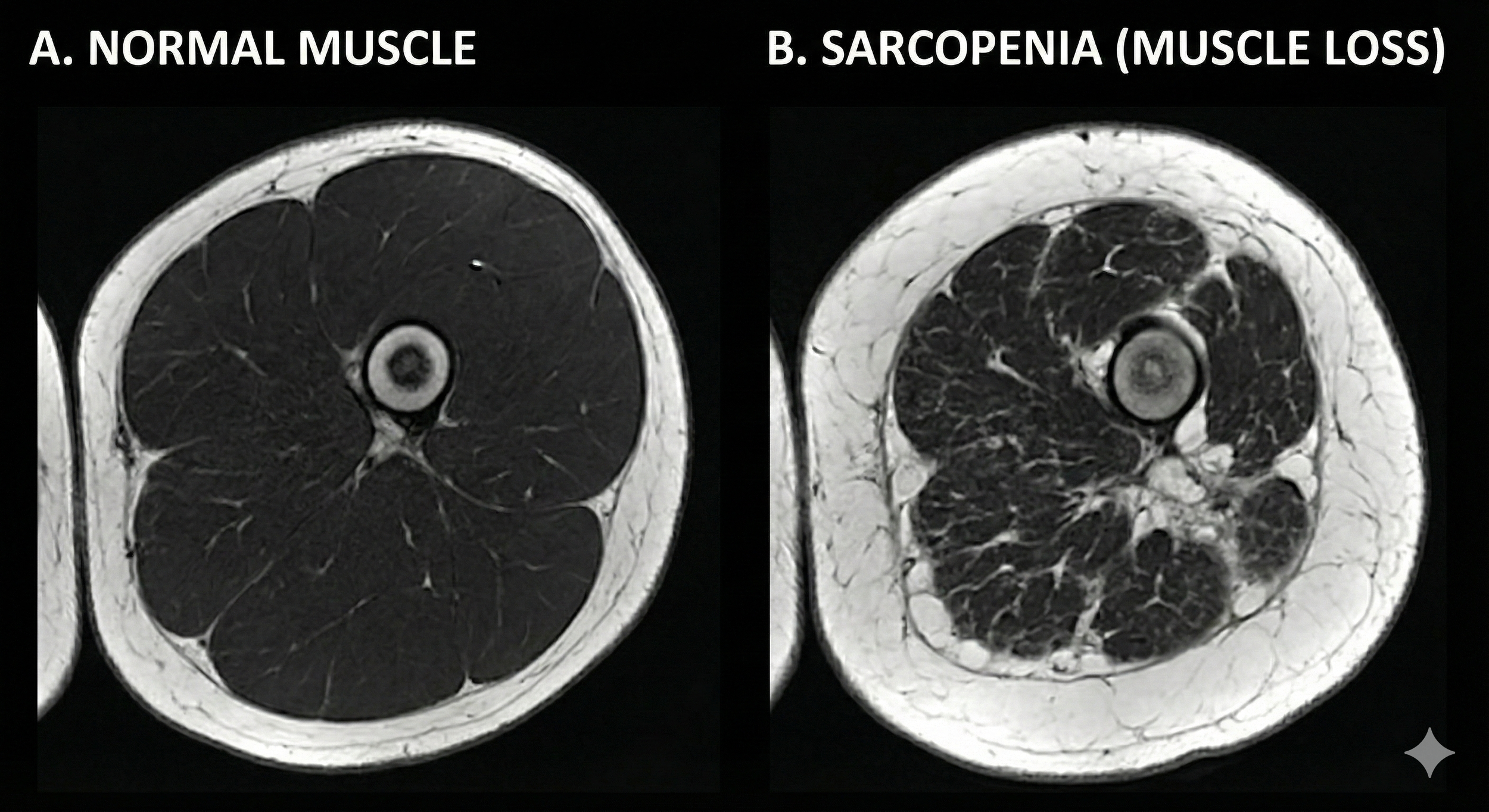
THE ANTI-SARCOPENIA WEAPON (Muscle = Bone)
Bone goes where muscle pulls. The connection is the "Mechanostat Theory." If you have Sarcopenia (muscle loss), you will have Osteoporosis.
Heavy Resistance Training: This is non-negotiable. The LIFTMOR Trial demonstrated that high-intensity resistance training is safe and effective for improving bone density in postmenopausal women with low bone mass [9].
The Neuro 20 Suit (WB-EMS): For patients too frail to lift heavy weights (or those with spinal instability), we utilize Whole-Body Electrical Muscle Stimulation (WB-EMS). Studies by Kemmler et al. have shown that WB-EMS significantly improves bone mineral density by creating intense muscle contractions without the joint impact [10].
Myostatin Inhibition (MYOS MD): We utilize Fortetropin®, a fertilized egg yolk isolate. Clinical trials indicate this compound lowers myostatin (the genetic brake on muscle growth), preserving the lean muscle mass required to exert tension on the skeleton [11].
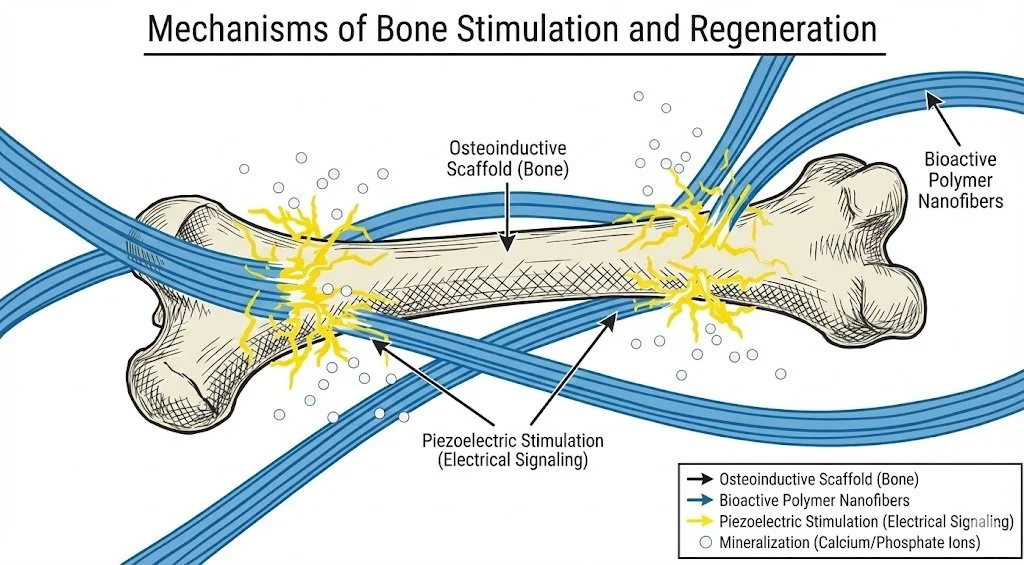
PHYSICS: THE PIEZOELECTRIC TRIGGER
We use physics to mimic the electrical signals of bone growth.
PEMF (Pulsed Electromagnetic Fields): PEMF therapy has a long history in orthopedics for healing non-union fractures. It works by stimulating the electrical potential of the osteoblast, signaling it to lay down new matrix [12].
Photobiomodulation (Red Light): Emerging literature suggests that PBM stimulates osteoblast proliferation and differentiation via mitochondrial ATP upregulation, effectively energizing the cells responsible for building bone [13].
THE METABOLIC AUDIT
Your skeleton does not exist in a vacuum.
Thyroid: We screen for hyperthyroidism, which accelerates bone turnover.
The Gut: We evaluate absorption. If you have inflammation (Leaky Gut), you cannot absorb the protein and minerals needed to build the matrix.
Steroid Sparing: Systemic steroids (Prednisone) are bone poison. They induce rapid apoptosis of osteoblasts. By using biohacking tools to manage autoimmune flares, we aim to reduce the patient's steroid burden, sparing the skeleton.
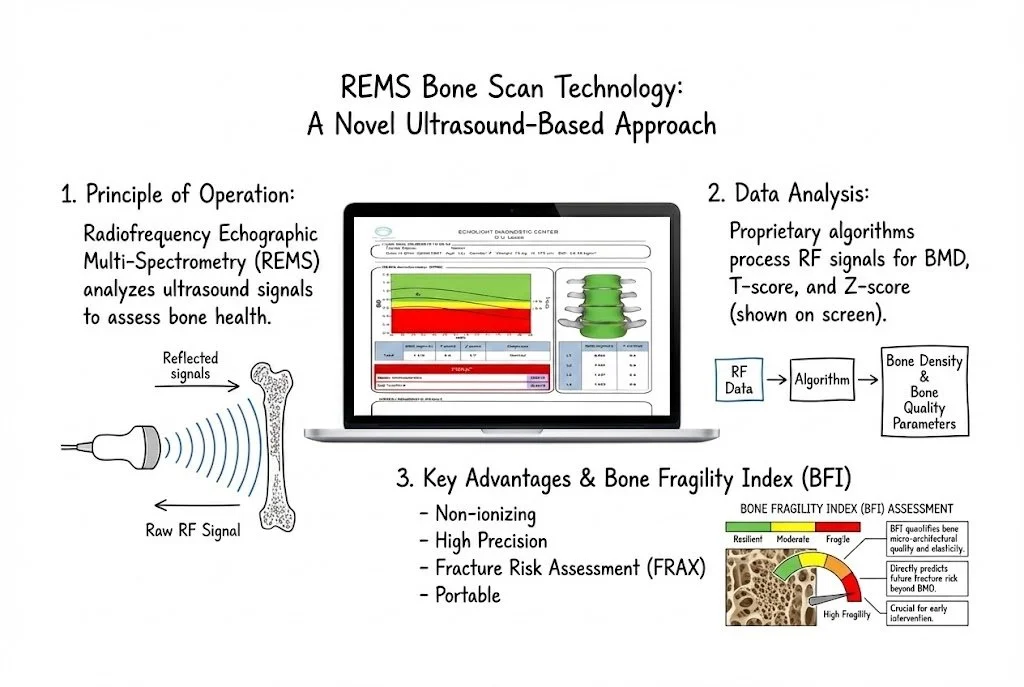
THE SCREENING REVOLUTION: ECHOLIGHT & REMS
The current standard (DEXA) has a fatal flaw: It uses X-ray radiation. Because of this, medical societies generally do not recommend screening women before age 65 (or 50 with risk factors). This is absurdist logic. I see women in their 30s with significant osteopenia due to stress, diet, and medications. By 50, the micro-architectural damage is often irreversible without aggressive drugs.
The Solution: Echolight Medical (REMS Technology) I serve on the Scientific Advisory Board of Echolight Medical because their technology solves the screening gap.
No Radiation: It uses Radiofrequency Echographic Multi-spectrometry (REMS)—an advanced form of ultrasound.
Fragility Score: Unlike DEXA, which only measures density (how much bone), REMS measures Micro-Architecture (how good the bone is).
Early Intervention: Because it is radiation-free, we can scan women in their 30s. If we catch osteopenia early, we can reverse it with lifestyle and engineering decades before drugs are required [14].
THE CONCLUSION
If you are worried about your future frailty, or if you have a family history of osteoporosis, do not wait for the "Standard of Care" to catch you when you fall. The goal is not just "dense" bone; it is Resilient Bone. It requires Muscle. It requires Hormones. It requires Physics. Come to the Lab. Get an Echolight REMS Scan. Let us engineer a frame that lasts as long as you do.
SCIENTIFIC BIBLIOGRAPHY
Leibson, C. L., et al. (2002). "Mortality, disability, and nursing home use for persons with and without hip fracture: a population-based study." Journal of the American Geriatrics Society.
Cooper, C. (1997). "The crippling consequences of fractures and their impact on quality of life." The American Journal of Medicine.
Gullberg, B., et al. (1997). "World-wide projections for hip fracture." Osteoporosis International.
DeWald, C. J., & Stanley, T. (2006). "Instrumentation-related complications of multilevel fusions for adult spinal deformity." Spine.
Fukada, E., & Yasuda, I. (1957). "On the piezoelectric effect of bone." Journal of the Physical Society of Japan.
Marx, R. E. (2003). "Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic." Journal of Oral and Maxillofacial Surgery.
Shane, E., et al. (2014). "Atypical subtrochanteric and diaphyseal femoral fractures: Second report of a task force of the American Society for Bone and Mineral Research." Journal of Bone and Mineral Research.
Snyder, P. J., et al. (2017). "Effect of Testosterone Treatment on Volumetric Bone Density and Strength in Older Men." JAMA Internal Medicine.
Watson, S. L., et al. (2018). "High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women with Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial." Journal of Bone and Mineral Research.
Kemmler, W., et al. (2016). "Whole-Body Electromyostimulation to Fight Osteopenia in Elderly Females: The Training and ElectroStimulation Trial (TEST-III)." Journal of Osteoporosis.
Evans, W., et al. (2020). "Effects of Fortetropin on the Rate of Muscle Protein Synthesis in Older Men and Women: A Randomized, Double-Blinded, Placebo-Controlled Study." Journal of Gerontology.
Bassett, C. A., et al. (1974). "Augmentation of bone repair by inductively coupled electromagnetic fields." Science.
Pinheiro, A. L., et al. (2001). "Light-emitting diode (LED) therapy in bone repair." Brazilian Dental Journal.
Adami, G., et al. (2020). "Radiofrequency echographic multi-spectrometry for the prediction of incident fragility fractures: A 5-year follow-up study." Bone.