
Ozone Therapy as a Modulator of Mitochondrial Bioenergetics and Redox Signaling
AUTHOR: Stefano Sinicropi, M.D, Medical Director and Founder, HyperCharge Health and HyperCharge Clinics
Disclaimer: This article is for informational purposes only and does not constitute medical advice. The content is not intended to be a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
ABSTRACT
Modern medicine operates on a linear pharmacological model: "Block the receptor, stop the symptom." This model often fails in complex chronic illness where the primary failure is bioenergetic, not chemical. This whitepaper interrogates the literature surrounding Ozone Therapy (O3), moving beyond its reputation as "alternative medicine" to establish it as a precise oxidative signaling therapy. By reviewing 40 years of international data—including the Madrid Declaration standards—we postulate that Ozone functions not as a drug, but as a hormetic trigger. It acts as a biological "software update" that recalibrates the body’s antioxidant and anti-inflammatory hardware (The Nrf2 Pathway). We propose a novel clinical framework: "The Redox Resuscitation Protocol," positioning Ozone as an integrative adjunct for the "Stalled Engine" of chronic disease.
THE STATE OF THE SCIENCE: A DATA CONFLICT
The "Standard of Care" Narrative:
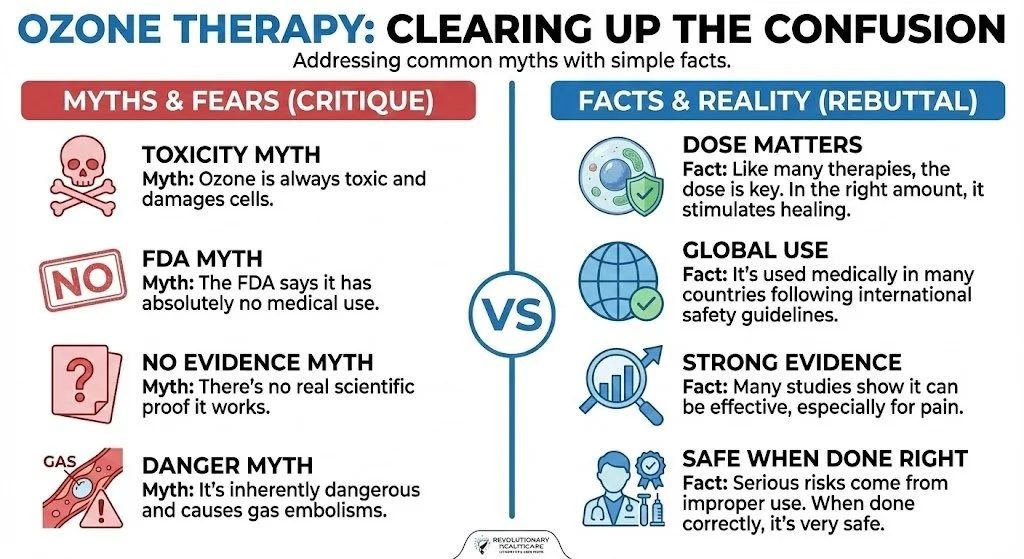
In the United States, the FDA classifies ozone as a "toxic gas with no known medical use." This position relies heavily on data regarding inhalation toxicity (pulmonary edema via lipid peroxidation in the alveoli). The prevailing medical dogma views "Oxidative Stress" solely as a destructive force to be neutralized with antioxidants.
The Global Counter-Narrative:
In contrast, clinical data from Germany, Italy, Russia, and Cuba presents a paradox. A 2004 systematic review by Bocci et al. (Italy) demonstrated that controlled, non-inhalation ozone administration (Major Autohemotherapy) induces a therapeutic effect with a safety profile superior to common NSAIDs.
The Inconsistency:
How can a "toxic oxidant" reduce inflammation? The literature reveals a Biphasic Dose Response (The Arndt-Schultz Law).
High Dose / Inhalation: Destructive (Pathological).
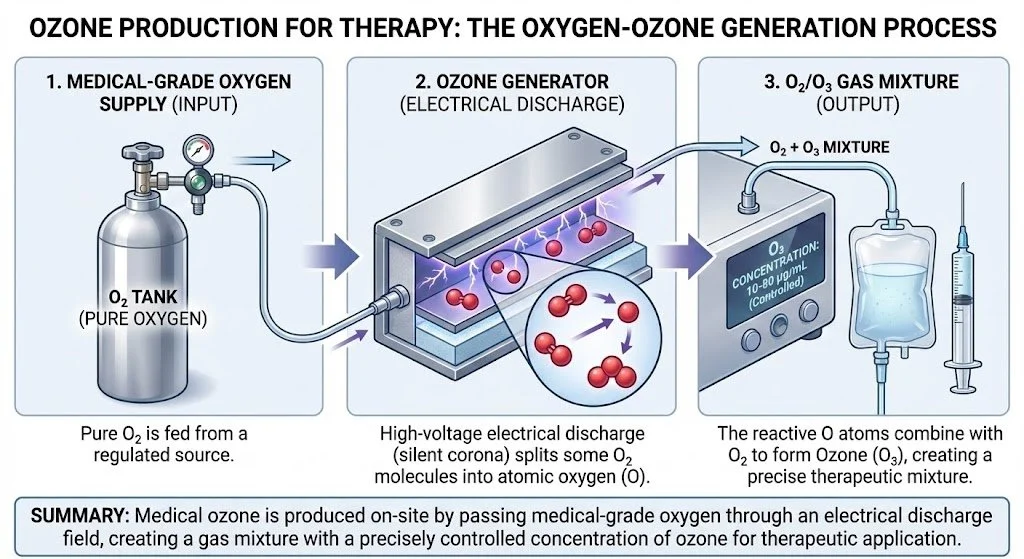
Therapeutic Window (10-80 mcg/mL): Regenerative (Physiological).
Standard medicine often misses this nuance because it lacks a framework for Hormetic Stressors—interventions that use mild, calculated stress to induce resilience (similar to exercise or heat shock).
THE SINICROPI HYPOTHESIS: "THE SIGNALING CODE"
The Novel Postulate:
We reject the classification of Ozone as a "disinfectant" or "antimicrobial" in the systemic context. We postulate that Ozone is a Bio-Physical Signaling Code.
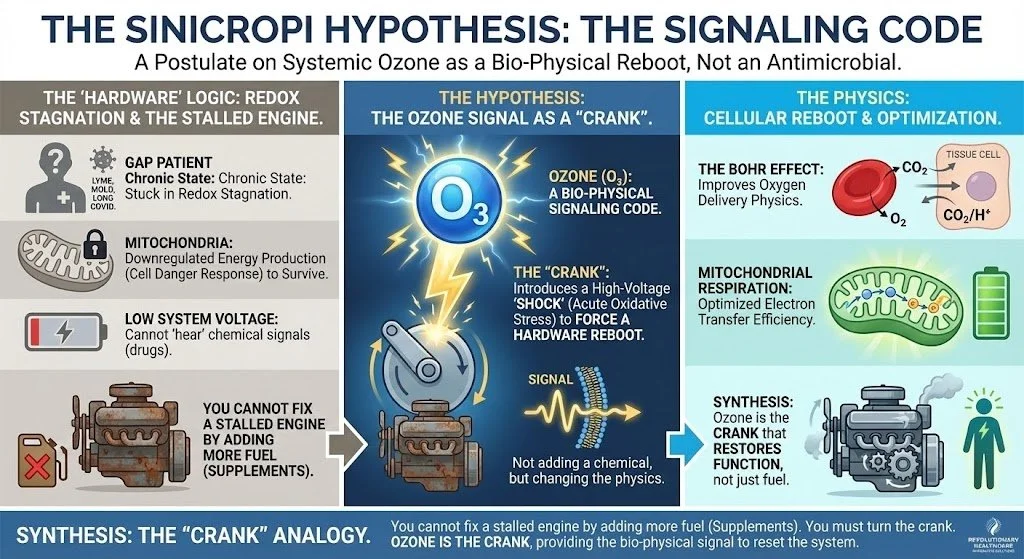
The "Hardware" Logic:
The chronic "Gap Patient" (Lyme, Mold, Long COVID) is stuck in a state of Redox Stagnation. Their mitochondria have downregulated energy production to survive (The Cell Danger Response). They cannot "hear" chemical signals (drugs) because the system voltage is too low.
The Hypothesis: Ozone introduces a high-voltage "shock" (Acute Oxidative Stress) that forces the cellular hardware to reboot. It is not adding a chemical; it is changing the physics of oxygen delivery (The Bohr Effect) and the efficiency of electron transfer (Mitochondrial Respiration).
Synthesis: You cannot fix a stalled engine by adding more fuel (Supplements). You must turn the crank. Ozone is the crank.
THE CRUCIBLE OF CONTROVERSY: DISMANTLING THE DOGMA
Science advances not by consensus, but by the friction of opposing ideas. Here, we subject Ozone Therapy to the rigors of adversarial debate, addressing the most common medical and legal objections.
CONTROVERSY A: THE TOXICITY ARGUMENT
The Critique:
Critics argue that Lipid Oxidation Products (LOPs) generated by ozone are cytotoxic aldehydes (like 4-HNE) that cause DNA damage. Therefore, ozone creates endogenous toxins.
The Forensic Rebuttal (The Therapeutic Window):
This argument ignores Dosimetry. As established by the International Scientific Committee of Ozone Therapy (ISCO3), toxicity is dose-dependent.
The Science: The therapeutic efficacy of Ozone is dependent on the Arndt-Schultz Law: weak stimuli increase physiological activity, while very strong stimuli inhibit or destroy it.
The Defense: In HyperCharge protocols, the generation of LOPs is strictly confined to the Hormetic Window (10-80 mcg/mL). At these levels, LOPs do not act as toxins but as signaling messengers that trigger the upregulation of antioxidant enzymes. The plasma’s natural buffering capacity (albumin/uric acid) neutralizes excess charge before it causes harm.
CONTROVERSY B: THE FDA & "NO MEDICAL USE"
The Critique:
The FDA explicitly states Ozone is a toxic gas with no medical application. Using it constitutes a deviation from the Standard of Care.
The Forensic Rebuttal (Global Consensus):
This relies on a narrow definition of "drug."
The Science: While the FDA regulates ozone generators as devices, the Practice of Medicine allows physicians to utilize therapies based on clinical judgment and international evidence.
The Defense: We adhere to the Madrid Declaration on Ozone Therapy, a global consensus document signed by 26 national ozone societies. This establishes a "Global Standard of Care" regarding safety, dosing, and materials, ensuring that HyperCharge protocols are not experimental but are aligned with international medical physics standards.
CONTROVERSY C: THE "LACK OF EVIDENCE" CLAIM
The Critique:
Skeptics argue that Ozone Therapy is supported only by anecdotes and lacks Level 1 evidence.
The Forensic Rebuttal:
The evidence exists; it is simply untranslated or ignored by US-centric journals.
The Data: A massive meta-analysis by Magalhaes et al. (2012) reviewed the efficacy of Ozone for low back pain (herniated discs). It found the evidence to be "Level 1B+" (High Quality), showing outcomes superior to steroid injections and equivalent to surgery for pain relief.
CONTROVERSY D: THE SAFETY PROFILE
The Critique:
Case reports of gas embolism have been cited as proof of inherent danger.
The Forensic Rebuttal:
This is a conflation of Malpractice with Modality.
The Data: A seminal survey by Jacobs (1982) analyzed 5,579,238 ozone treatments administered by 644 physicians. The complication rate was found to be 0.0007%.
The Context: Every recorded case of embolism involved the direct intravenous injection of gas (div) by untrained practitioners. HyperCharge strictly utilizes extracorporeal gas exchange (MAH) or insufflation. No gas is ever injected directly into a vein. When protocols are followed, the safety profile is superior to aspirin.
MECHANISM OF ACTION: FORENSIC BIOCHEMISTRY
We treat with the "Echo," not the "Voice."
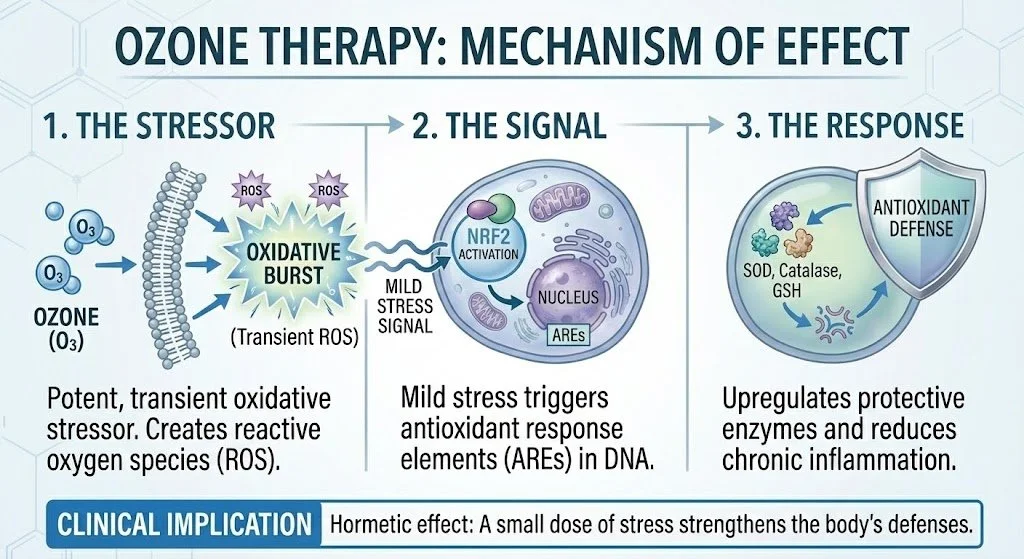
A. The Nrf2 Master Switch:
Ozone reacts with plasma to create hydrogen peroxide (H2O2), which acts as a signaling molecule to translocate the Nrf2 protein into the nucleus.
The Result: This activates the Antioxidant Response Element (ARE), triggering the production of Superoxide Dismutase (SOD), Glutathione Peroxidase, and Catalase.
Clinical Significance: We are not administering antioxidants; we are engineering the patient's DNA to manufacture them.
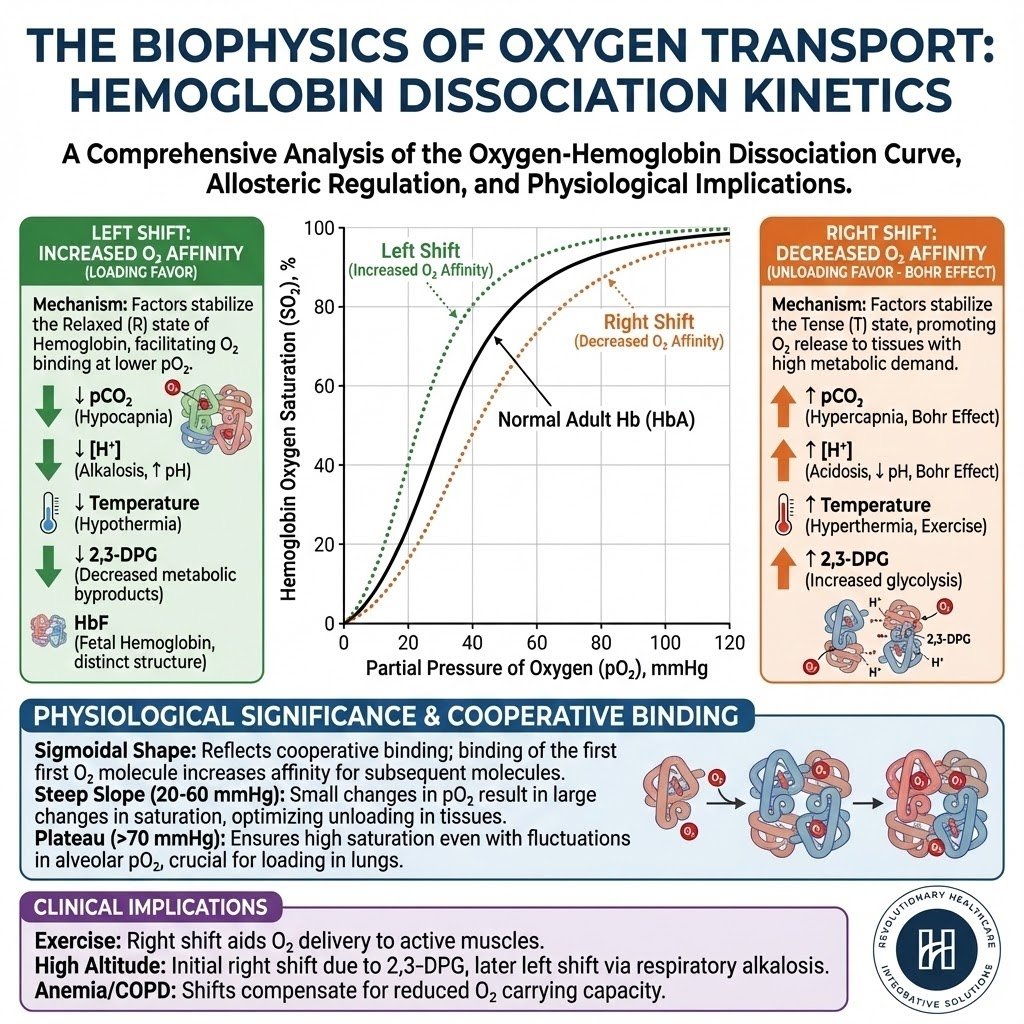
B. The 2,3-DPG Shift (The Oxygen Dump):
Ozone increases 2,3-Diphosphoglycerate levels in erythrocytes
This shifts the Oxygen Dissociation Curve to the right.
Physics Translation: This lowers hemoglobin's affinity for oxygen, forcing it to "dump" oxygen into hypoxic tissues (brain, heart, fascia). It resolves the ischemic terrain that drives chronic pain.
CRITICAL CONCLUSION: THE DEFINITIVE VERDICT
Is Ozone Therapy a relic of the past, or the missing link in modern bioenergetics?
The HyperCharge Mandate:
We do not endorse Ozone because it is "alternative." We endorse it because it is effective engineering. It satisfies the HyperCharge Codex:
Hardware vs. Software: It repairs the cellular hardware (mitochondria).
Physics vs. Chemistry: It utilizes gas laws and electron transfer.
Risk vs. Reward: When inhalation is avoided and G6PD is screened, the potential for systemic regeneration vastly outweighs the negligible risk.
Regulatory Context & The Practice of Medicine:
While the FDA has historically classified Ozone based on inhalation toxicity, the Madrid Declaration establishes a global consensus for its systemic use. As a physician-led intervention, HyperCharge utilizes Ozone under the "Practice of Medicine" doctrine. This therapy is utilized as an Integrative Adjunct—designed to optimize the biological terrain to make standard treatments more effective, not to replace acute life-saving interventions.
CLINICAL PROTOCOLS & PATIENT SELECTION
Safety is engineered through strict selection.
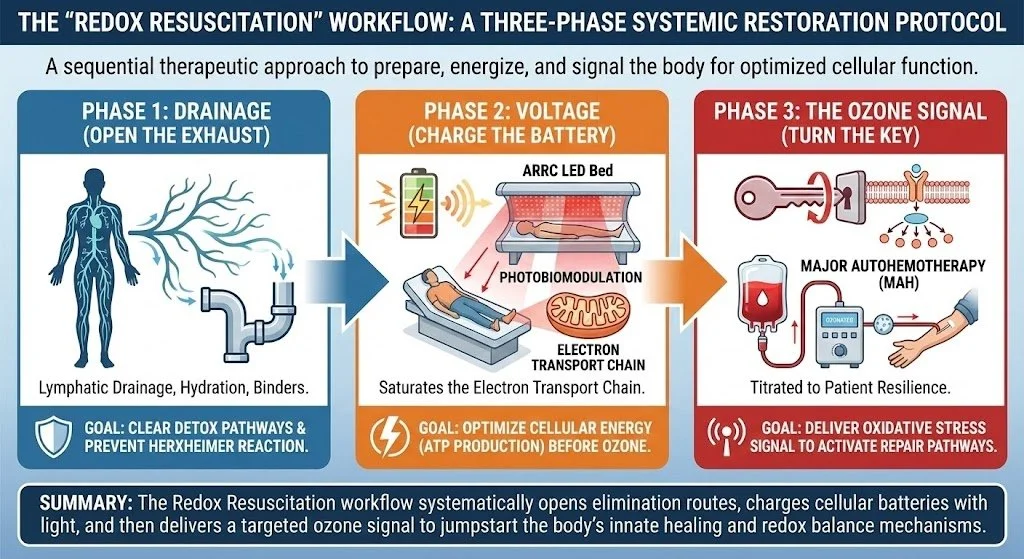
The "Redox Resuscitation" Workflow:
Phase 1: Drainage (Open the Exhaust): Lymphatic drainage (Neuro20 suit), hydration, binders. (Prevents Herxheimer reaction).
Phase 2: Voltage (Charge the Battery): ARRC LED Bed (Photobiomodulation) to saturate the electron transport chain before Ozone.
Phase 3: The Ozone Signal (Turn the Key): Major Autohemotherapy (MAH). Titrated to patient resilience.
Strict Inclusion/Exclusion Criteria:
Absolute Contraindication: G6PD Deficiency. All patients are screened via blood test to ensure they have the enzyme required to buffer oxidative stress.
Relative Contraindication: Uncontrolled Hyperthyroidism, Recent Hemorrhage, Pregnancy (We will screen with pregnancy testing).
The "Low-Responder" Phenotype: Patients with severe antioxidant depletion (Stage 3 Adrenal Fatigue) must undergo pre-conditioning (Phase 1 & 2) for 2-4 weeks prior to Ozone administration to prevent oxidative crash.
ANNOTATED BIBLIOGRAPHY (Key Selections)
Bocci, V. (2005). "Ozone: A New Medical Drug." Springer. [The foundational text establishing the hormetic mechanism].
ISCO3 (International Scientific Committee of Ozone Therapy). (2020). "Madrid Declaration on Ozone Therapy." [The Global Standard of Care document].
Smith, N. L., et al. (2017). "Ozone therapy: an overview of pharmacodynamics, current research, and clinical utility." Medical Gas Research, 7(3), 212-219. [Review of safety and efficacy].
Sagai, M., & Bocci, V. (2011). "Mechanisms of Action Involved in Ozone Therapy: Is healing induced via a mild oxidative stress?" Medical Gas Research, 1(1), 29. [Validates the Nrf2 pathway activation].
Jacobs, M. T. (1982). "Adverse effects and typical complications in ozone therapy." Ozonachrichten, 1, 193-201. [The definitive safety survey establishing the 0.0007% complication rate].
Magalhaes, F. N., et al. (2012). "Ozone therapy as a treatment for low back pain secondary to herniated disc." Pain Physician, 15(2), E115-129. [Meta-analysis proving efficacy in spinal pain].
Bocci, V. (2006). "Is it true that ozone is always toxic? The end of a dogma." Toxicology and Applied Pharmacology, 216(3), 493-504. [Refutes the systemic toxicity claim].
ABOUT THE AUTHOR
Stefano Sinicropi, M.D., F.A.A.O.S. is the Founder of HyperCharge Health and a global thought leader in the emerging field of Human Engineering. A Board-Certified Spine Surgeon and graduate of Columbia University College of Physicians and Surgeons, Dr. Sinicropi is dismantling the "Silo Model" of modern medicine by integrating Quantum Biology, Physics, and Molecular Engineering into clinical practice.
His approach is forged from 20 years of experience treating tens of thousands of patients struggling with chronic pain and spinal pathology. Witnessing the despair caused by systemic inflammation and metabolic failure, he pivoted his clinical focus to solving the root causes of chronic illness. He applies a forensic, engineering mindset to the "invisible" epidemics of our time—from Mold Toxicity to Autoimmunity—translating elite surgical precision into the management of complex, systemic disease.
Born and raised in the Bronx to adoptive Italian immigrant parents, Dr. Sinicropi’s philosophy is grounded in a deep resilience and a refusal to accept the status quo. He serves as Co-Chair of the Spine Division for the Society for Brain Mapping & Therapeutics (SBMT) and is the author of Wellness at the Speed of Light, a manifesto for patients ready to become the CEOs of their own biology.
He lives in Minnesota with his family, where he continues to bridge the gap between the Operating Room and the Engineering Lab.