
Restoring the Terrain in Mold Illness - Chronic Inflammatory Response Syndrome (CIRS): Beyond Functional Biochemical Detoxification
By Dr. Stefano Sinicropi, Founder of HyperCharge Health
Disclaimer: This blog is for informational purposes only and does not constitute medical advice. The content is not intended to be a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Chronic Inflammatory Response Syndrome (CIRS), commonly known as "Mold Illness," acquired from exposure to water-damaged buildings (WDB), represents a catastrophic failure of the innate immune system and cellular bioenergetics. The current integrative standard of care—Functional Medicine utilizing the Shoemaker Protocol—relies predominantly on biochemical interventions: systemic binders, targeted supplements, and dietary modulation to facilitate detoxification. While diagnostically precise and biochemically sound, this approach frequently encounters significant clinical ceilings in chronic, multisystemic cases. These limitations stem from a fundamental oversight: the inability of a metabolically exhausted host with compromised membrane transport and lymphatic stasis to execute complex biochemical detoxification pathways. This review argues for a paradigm shift toward a "Physics-First" hierarchy of care. By prioritizing advanced biophysical modalities—specifically Photobiomodulation (PBM), Hyperbaric Oxygen Therapy (HBOT) combined with Exercise with Oxygen Therapy (EWOT), Pulsed Electromagnetic Field (PEMF) therapy, and mechanical lymphatic/glymphatic clearance—clinicians can address the structural and energetic pathologies of CIRS that chemical agents cannot reach. We propose that restoring cellular voltage, reducing tissue hypoxia, and mechanically forcing detoxification pathways is the essential prerequisite for biochemical interventions to be effective.
The Hidden Epidemic of Innate Immune Failure
Exposure to water-damaged buildings (WDB) and the resultant microbial milieu—including fungi, bacteria, actinomycetes, and their metabolic byproducts (mycotoxins, endotoxins, inflammagens)—is an escalating public health crisis. The World Health Organization estimates that up to 50% of buildings in North America have some degree of dampness sufficient to promote microbial growth [1].
For a genetically susceptible subset of the population (approximately 24% carrying specific HLA-DR haplotypes), exposure to these biotoxins does not trigger a typical allergic response, but rather a runaway, chaotic activation of the innate immune system known as Chronic Inflammatory Response Syndrome (CIRS) [2].
CIRS is not an allergy; it is genomic instability driven by chronic inflammation. It is characterized by multisystemic dysregulation, including neurocognitive decline ("mold brain"), profound fatigue, respiratory distress, and autonomic nervous system collapse (POTS/dysautonomia).
As an orthopedic surgeon focused on regenerative medicine, I view CIRS through a lens of structural and energetic failure. The prevailing Functional Medicine model views CIRS as a "toxicity" problem to be solved with chemical binders. While true, this ignores the reality that detoxification is an energy-expensive physiological process. A body in a state of mitochondrial collapse cannot detoxify. This review contends that the failure to treat chronic CIRS effectively stems from relying on biochemical inputs for what has become a biophysical collapse. To understand the necessity of biohacking, we must first dissect the pathophysiology of CIRS and the limitations of the current chemical standard of care.
The Pathophysiology of CIRS: The Enemy Within
To treat mold illness, one must understand that the pathogen is not alive; it is a biotoxin that triggers a genomic cascade.
The Failure of Antigen Presentation
In healthy individuals, mycotoxins entering the body are identified by the adaptive immune system, tagged by antibodies, and eliminated. In genetic CIRS patients, the HLA-DR receptors on antigen-presenting cells fail to "see" the biotoxin structure. The adaptive immune system never gets involved.
The Innate Immune Cascade (The Cytokine Storm)
Because the biotoxins are not cleared, they remain circulating indefinitely. The innate immune system, sensing a constant threat it cannot eliminate, remains perpetually activated. This results in a massive, unordered release of inflammatory cytokines (TGF-beta1, MMP-9, IL-1B) and complement inflammatory responses (C4a, C3a) [3].

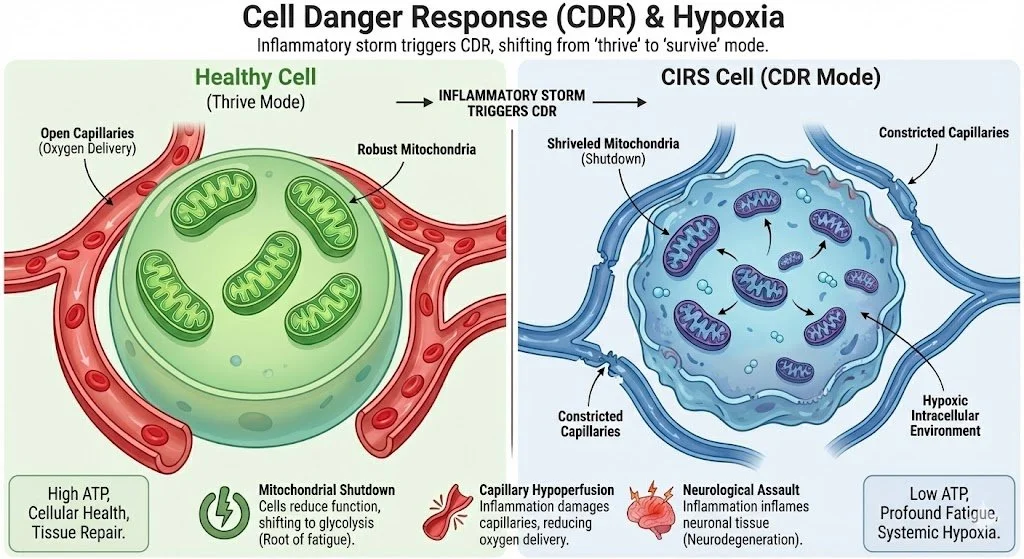
The Consequence: "Cell Danger Response" and Hypoxia
This inflammatory storm triggers what Dr. Robert Naviaux terms the "Cell Danger Response" (CDR). The body shifts resources from "thrive" modes (energy production, repair) to "survive" mode (defense).
Mitochondrial Shutdown: To prevent the spread of perceived pathogens, cells voluntarily reduce mitochondrial function, shifting from efficient aerobic respiration to inefficient glycolysis. This is the root of the profound fatigue in CIRS.
Capillary Hypoperfusion: High levels of cytokines, particularly MMP-9 and C4a, damage capillary beds and cause vasoconstriction. This reduces oxygen delivery to tissues, creating systemic hypoxia, even if the patient is breathing normally [4].
Neurological Assault: Inflammation degrades the Blood-Brain Barrier (BBB), allowing toxins and cytokines to inflame neuronal tissue, leading to neuroexcitation (anxiety, insomnia) followed by neurodegeneration (cognitive decline).
The Standard of Care (Functional Medicine) & Its Limitations
Dr. Ritchie Shoemaker pioneered the understanding and treatment of CIRS. The "Shoemaker Protocol" and subsequent Functional Medicine adaptations rely on a logical, stepwise biochemical approach:
Remove exposure (remediation/avoidance).
Utilize anionic resin binders (Cholestyramine, Welchol) to trap biotoxins in the bile and excrete them in stool.
Correct hormonal and inflammatory markers with supplements (VIP spray, fish oils, etc.).
While this protocol is the foundation of modern CIRS treatment, it frequently hits a clinical ceiling in severely chronic cases. The limitation is not the theory, but the host's capacity to execute the theory.
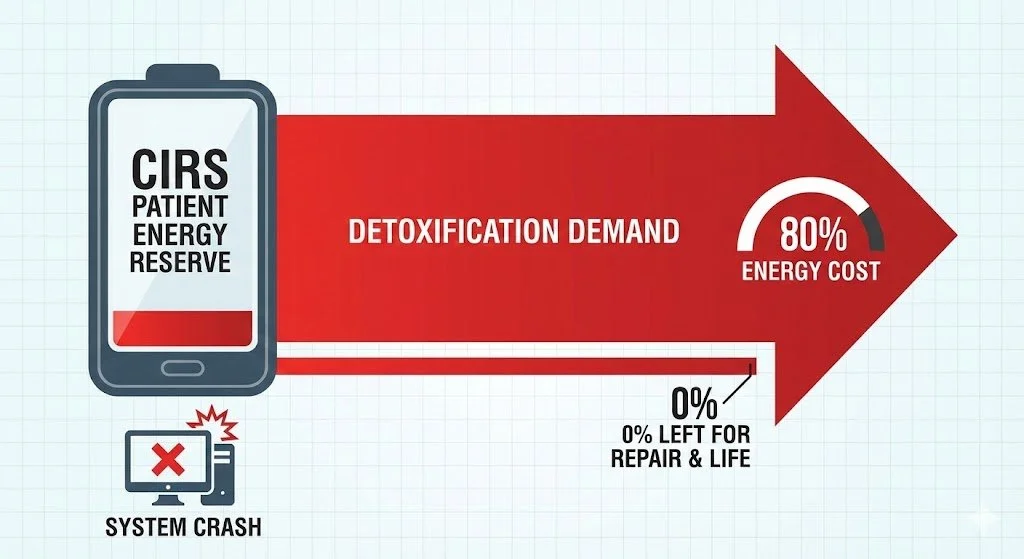
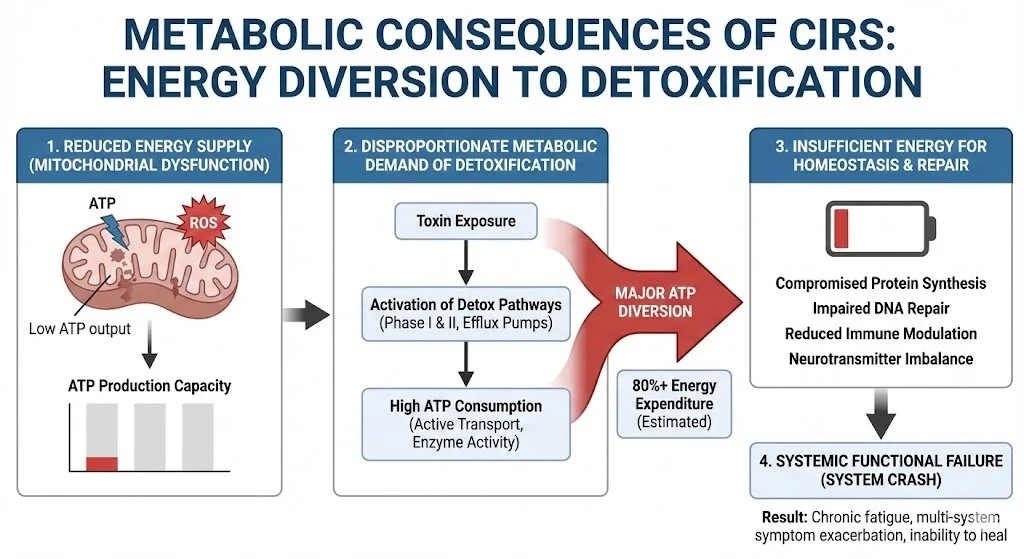
The "Metabolic Tax" of Detoxification
Detoxification is not passive. Phase I and II hepatic detoxification pathways, the synthesis of glutathione, and the active transport of toxins across cell membranes are all heavily ATP-dependent processes. CIRS patients are in mitochondrial failure. Asking a patient with no cellular energy to undertake an aggressive detoxification protocol is equivalent to asking a starving person to run a marathon. The "Metabolic Tax" of processing binders and mobilizing toxins often crushes the patient, leading to severe exacerbations.
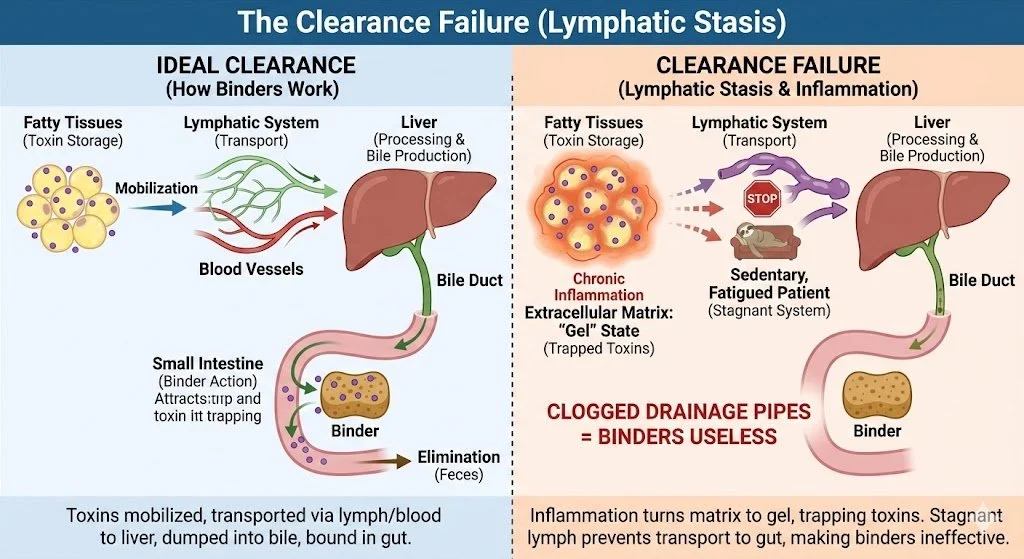
The Clearance Failure (Lymphatic Stasis)
Binders only work in the small intestine. They rely on the body's ability to mobilize toxins from fatty tissues, transport them via the lymph and blood to the liver, and dump them into the bile. Chronic inflammation causes the extracellular matrix to turn from a fluid "sol" state to a gelatinous "gel" state, trapping toxins. Furthermore, sedentary, fatigued patients have stagnant lymphatic systems. If the "drainage pipes" leading to the gut are clogged, binders sitting in the gut are useless.
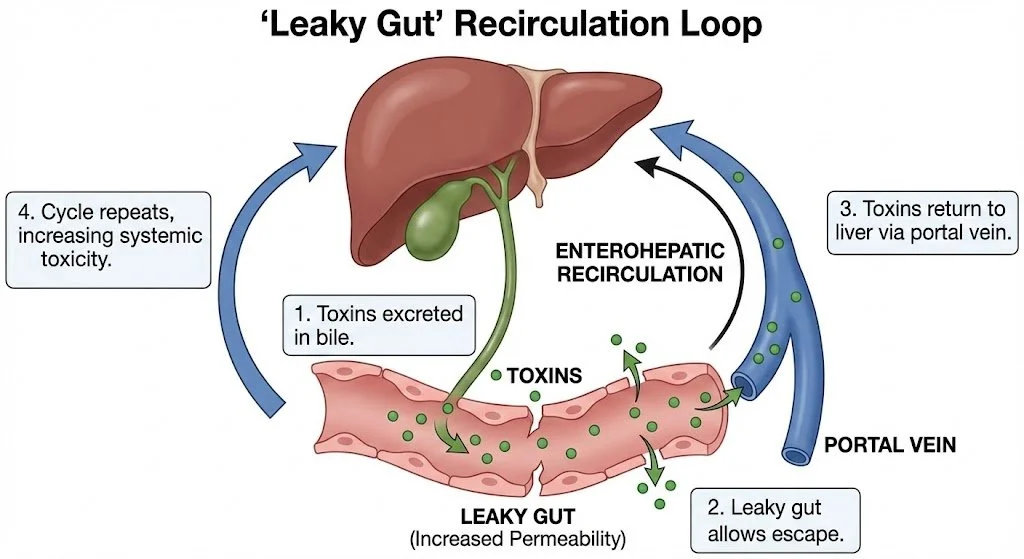
The "Leaky Gut" Recirculation Loop
CIRS almost universally causes intestinal hyperpermeability (leaky gut) due to MSH (Melanocyte-Stimulating Hormone) deficiency and direct toxin damage [5]. Even if a binder catches a toxin in the bile, a compromised gut barrier allows the toxin-binder complex, or free toxins, to leak back into the portal bloodstream before they can be excreted. This creates a futile loop of enterohepatic recirculation, rendering the therapy inefficient and increasing systemic toxicity.
The Biophysical Imperative: Why Physics Precedes Chemistry
To overcome these limitations, we must shift the paradigm from "chemical detoxification" to "biophysical restoration." We must repair the machine before we expect it to process the fuel.
Biohacking modalities utilize the fundamental forces of physics—light, oxygen, magnetism, and mechanics—to alter the biological terrain without relying on the compromised digestive or metabolic systems of the host. These modalities are net-positive energy donors.
The Hierarchy of Healing in CIRS:
Physics (Foundation): Restore voltage, oxygen tension, and drainage flow.
Chemistry (Structure): Utilize binders and nutrients to remove mobilized toxins.
Biology (Function): The immune system resets.
Advanced Modalities: Mechanisms of Action in CIRS
The following modalities address the specific pathophysiological failures of CIRS that biochemical protocols miss.
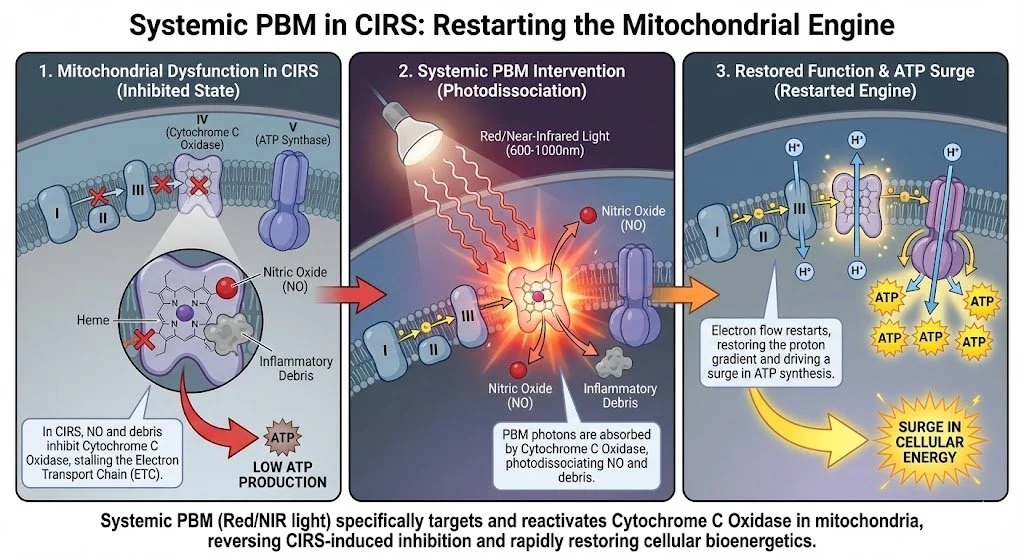
Photobiomodulation (PBM): Restarting the Cellular Engines
The Problem: Mitochondrial hibernation (Cell Danger Response) halts the energy needed for detoxification.
The Biophysical Solution: Systemic PBM (Red/Near-Infrared light) targets Cytochrome C Oxidase in the mitochondria. In CIRS, this enzyme is often inhibited by nitric oxide or inflammatory debris. PBM photodissociates these inhibitors, instantly restarting the electron transport chain and surging ATP production [6].
`CIRS Application: PBM provides the exogenous energy required to fuel hepatic detoxification pathways and power immune cell function, without creating a metabolic tax on the patient.
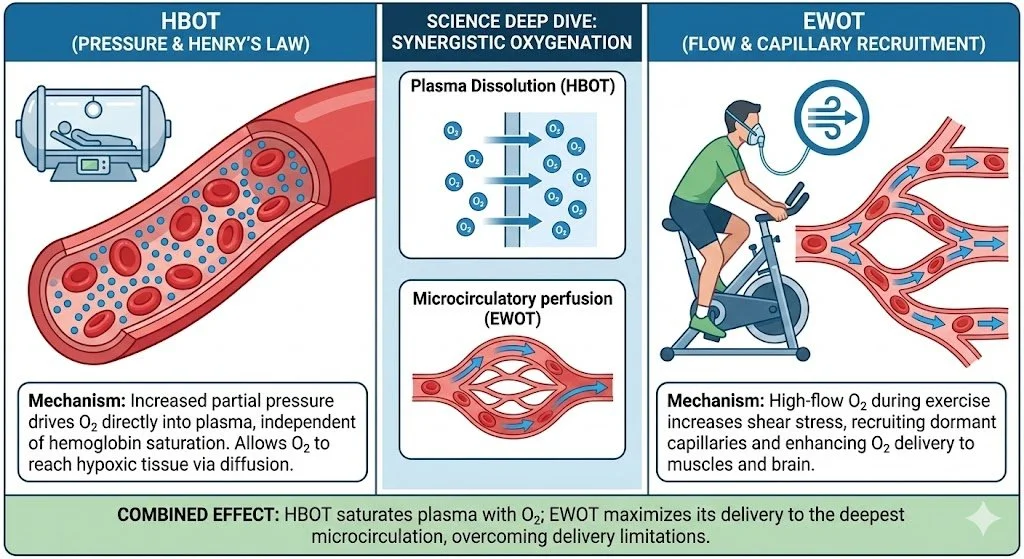
Hyperbaric Oxygen (HBOT) & Exercise With Oxygen Therapy (EWOT): The Synergistic Oxidative Strike
The Problem: CIRS causes "capillary hypoperfusion." High levels of C4a and MMP-9 damage capillary beds and cause vasoconstriction. This leads to deep tissue hypoxia, which fuels inflammation and allows anaerobic organisms to thrive.
The Biophysical Solution: At HyperCharge, we utilize a dual-oxygen approach to overcome this perfusion barrier.
Hyperbaric Oxygen Therapy (HBOT): HBOT utilizes Henry’s Law to dissolve oxygen directly into the plasma, bypassing compromised hemoglobin transport. This hyper-oxygenated plasma can seep into tissues where capillaries are damaged or constricted.
Nrf2 Activation: HBOT activates the Nrf2 genetic pathway, the body's master regulator of endogenous antioxidant production (Superoxide Dismutase, Glutathione) [7]. This provides internal protection against the oxidative stress of toxin mobilization.
Exercise With Oxygen Therapy (EWOT): While HBOT drives oxygen deep via pressure, EWOT drives oxygen via flow and turbulence. Based on the work of Manfred von Ardenne, EWOT involves exercising (to increase cardiac output) while breathing high-concentration oxygen.
Vasodilation: The CO2/O2 exchange gradient during EWOT forces the opening of distal capillaries that are often shut down in CIRS.
Anti-Inflammatory Flush: The massive influx of oxygenated blood acts as a "pressure wash" for the endothelium, reducing vascular inflammation and restoring functional perfusion [8].
Pulsed Electromagnetic Field (PEMF): Liberating Sequestered Toxins
The Problem: Mycotoxins are lipophilic (fat-loving) and sequester themselves inside cells and fatty tissues. Chronic inflammation reduces cell membrane voltage, locking ion channels and trapping toxins inside.
The Biophysical Solution: PEMF restores the transmembrane potential (-70mV to -90mV). This "electroporation" opens cell ion channels, allowing nutrients to enter and, most importantly, allowing sequestered intracellular toxins to be expelled into the extracellular space, where they can finally be transported to the liver for binding [9].
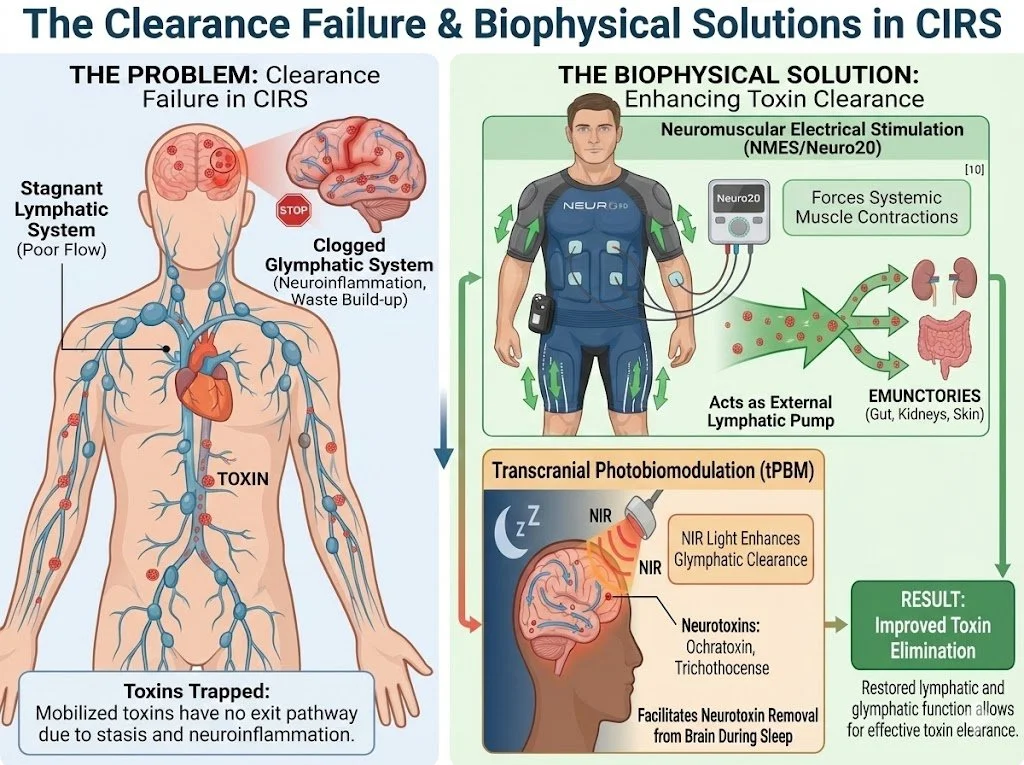
Mechanical Drainage: Lymphatics and the Glymphatic System
The Problem: Toxins mobilized from cells need a pathway to the exit. In CIRS, the lymphatic system is stagnant, and the brain's waste clearance system (the Glymphatic System) is clogged due to neuroinflammation.
The Biophysical Solution:
Neuromuscular Electrical Stimulation (NMES/Neuro20): By forcing systemic muscle contractions, NMES acts as an external pump for the lymphatic system, moving stagnant, toxin-laden lymph toward emunctories [10].
Transcranial Photobiomodulation (tPBM): Recent research indicates that NIR light applied to the head can enhance glymphatic clearance, facilitating the removal of neurotoxins like ochratoxin and trichothecenes from the brain parenchyma during sleep [11].
Vagus Nerve Stimulation & TMS: Resetting the Alarm
The Problem: The limbic system and autonomic nervous system (ANS) in CIRS patients are stuck in a "sympathetic freeze" (fight or flight), contributing to POTS and anxiety. A body in high-threat mode will not prioritize detoxification (a parasympathetic process).
The Biophysical Solution: Neuromodulation techniques like Transcranial Magnetic Stimulation (TMS) and auricular Vagus Nerve Stimulation (VNS) electrically signal safety to the brainstem and limbic system. By shifting the ANS toward parasympathetic dominance ("rest and digest"), we open the physiological windows necessary for healing and detoxification to occur.
Synthesis: The Integrated Protocol
A successful CIRS protocol must sequence physics before chemistry to avoid overwhelming the host.
Phase 1: The Biophysical Foundation (4-8 Weeks)
Goal: Stabilize energy, open drainage pathways, reduce systemic hypoxia. No aggressive binders yet.
Modalities: Systemic/Transcranial PBM (energy), EWOT (perfusion), Lymphatic drainage (Neuro20 + Transcranial PBM), VNS (autonomic balance).
Phase 2: Mobilization and Binding (Ongoing)
Goal: Liberate sequestered toxins and bind them in the gut.
Modalities: Add PEMF (cellular release) and EWOT (Nrf2/Detox support) immediately prior to binder administration. Continue Phase 1 support to process the mobilized load.
Phase 3: Regeneration (Post-Detox)
Goal: Repair tissue damage from years of inflammation.
Modalities: PBM, EWOT, PEMF, Peptides, Supplements for stem cell mobilization to repair capillary beds and neurological damage.
The Paradigm Shift in Environmental Medicine
Chronic Inflammatory Response Syndrome is a definitive pathology of the 21st century—an interaction between environmental toxicity and genetic susceptibility that breaks the fundamental energy mechanisms of the human body.
The functional medicine approach of "detect and bind" is necessary but often insufficient in chronic, metabolically shattered patients. We have been attempting to perform complex biochemical operations on a patient lacking the biophysical currency to pay for them.
By integrating regenerative biohacking, we are not merely adding "adjunct therapies." We are addressing the prerequisite conditions for healing. We are restoring the voltage, the oxygen, and the flow that allow the chemistry of life—and the chemistry of detoxification—to function. In the treatment of mold illness, physics is not optional; it is imperative.
Bibliography
World Health Organization. (2009). WHO Guidelines for Indoor Air Quality: Dampness and Mould.
Shoemaker, R. C., & House, D. E. (2006). Sick building syndrome (SBS) and exposure to water-damaged buildings: time series study, clinical trial and mechanisms. Neurotoxicology and Teratology, 28(5), 573-588.
Shoemaker, R. C., et al. (2010). Innate immunity, MR spectroscopy, HLA DR, TGF beta-1, VIP and capillary hypoperfusion define acute and chronic human illness acquired following exposure to water-damaged buildings. Health, 2(7), 723-731.
Naviaux, R. K. (2014). Metabolic features of the cell danger response. Mitochondrion, 16, 7-17.
Fasano, A. (2012). Leaky gut and autoimmune diseases. Clinical Reviews in Allergy & Immunology, 42(1), 71-78.
Hamblin, M. R. (2017). Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophysics, 4(3), 337-361.
Thom, S. R. (2009). Oxidative stress is fundamental to hyperbaric oxygen therapy. Journal of Applied Physiology, 106(3), 988-995.
von Ardenne, M. (1990). Oxygen Multistep Therapy: Physiological and Technical Foundations. Thieme.
Oschman, J. L. (2000). Energy Medicine: The Scientific Basis. Churchill Livingstone.
Olszewski, W. L. (2003). The lymphatic system in body homeostasis: physiological conditions. Lymphatic Research and Biology, 1(1), 11-21.
Salehpour, F., et al. (2022). Photobiomodulation therapy and the glymphatic system: Promising applications for augmenting brain waste clearance. International Journal of Molecular Sciences, 23(6), 2923.