
Patient Education Articles
Read our patient education articles below. Use the search bar below or click on a specific topic that interests you!
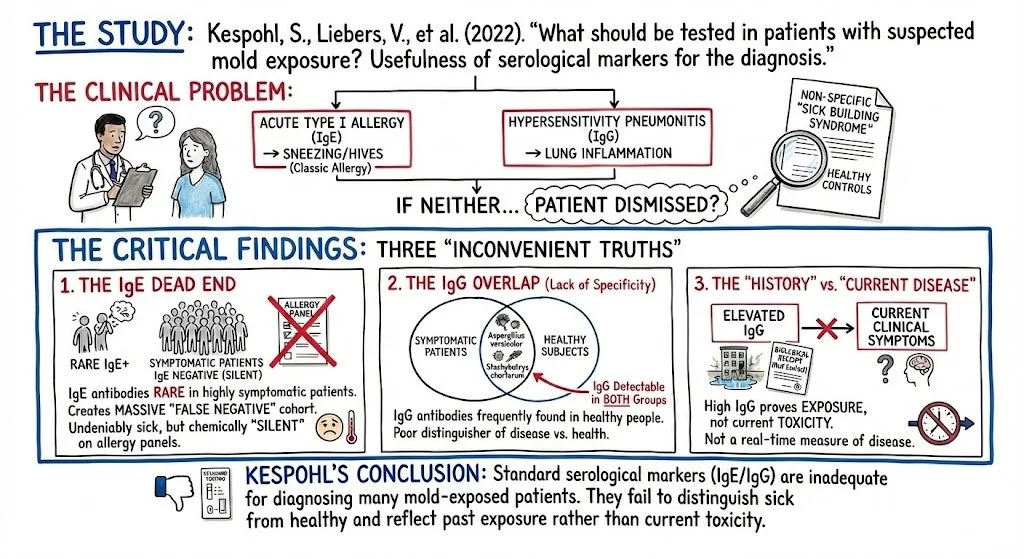
The Diagnostic Blind Spot: The Systemic Failure to Identify Mold Biotoxin Illness
The failure to diagnose Mold Biotoxin Illness is not merely a clinical oversight; it is a systemic error with devastating neuro-immune consequences. Current "Standard of Care" protocols rely almost exclusively on IgE (Allergy) and IgG (Exposure) serology. This binary approach creates a massive "Diagnostic Blind Spot": it correctly identifies the allergic patient but renders the septic, neuro-toxic patient invisible.
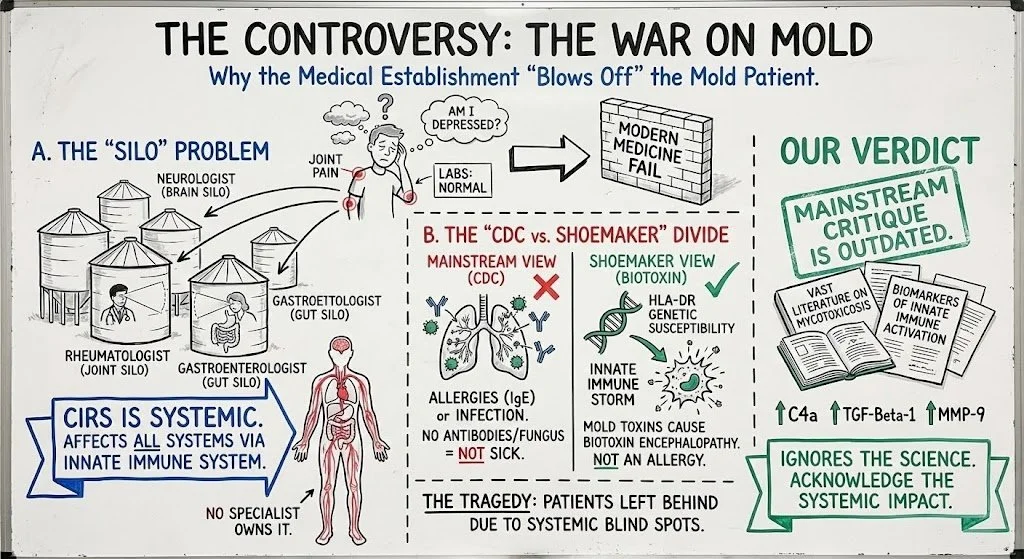
The Shoemaker Protocol: A Forensic Audit of the Standard of Care for Biotoxin Illness
For decades, a schism has existed in medicine regarding Mold Toxin Illness. On one side stands the mainstream medical establishment, which largely views mold exposure solely as an allergic or pulmonary event. On the other stands Dr. Ritchie Shoemaker, a primary care physician who mapped a distinct, multi-system pathology termed Chronic Inflammatory Response Syndrome (CIRS).
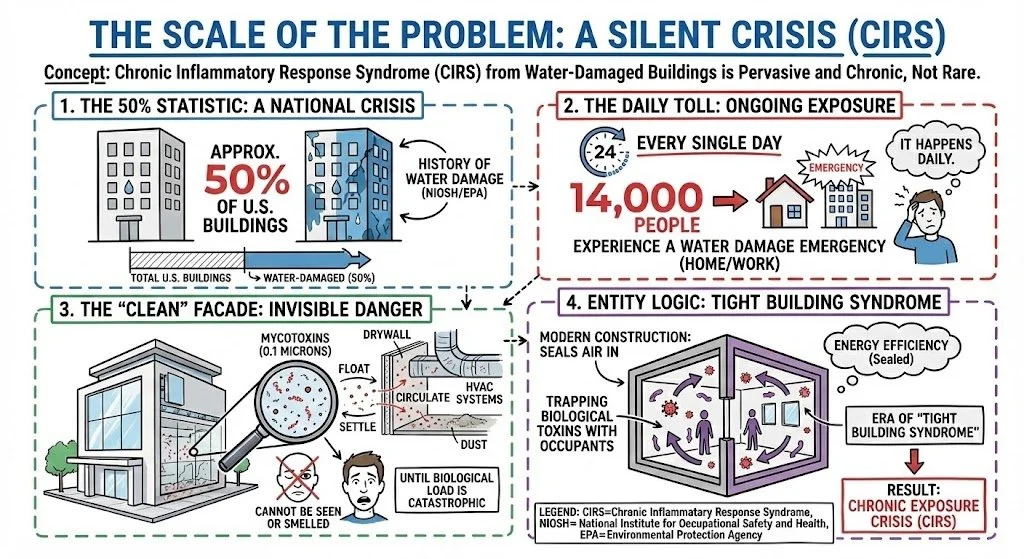
The Invisible Epidemic: Why Water Damage is the Most Overlooked Cause of Chronic Illness
The term "Mold Illness" is a misnomer. It suggests a rare, acute reaction. The reality is a pervasive, chronic exposure crisis known clinically as Chronic Inflammatory Response Syndrome (CIRS) acquired from water-damaged buildings.

The Moldy Brain: Why Psychiatric Symptoms are Often Environmental Toxicity
Every day, patients walk into clinics with a constellation of symptoms: panic attacks, sudden rage, brain fog, and treatment-resistant depression. They are prescribed SSRIs, Benzodiazepines, and Antipsychotics. They rarely get better. Why? Because they do not have a serotonin deficiency. They have a toxicity problem.
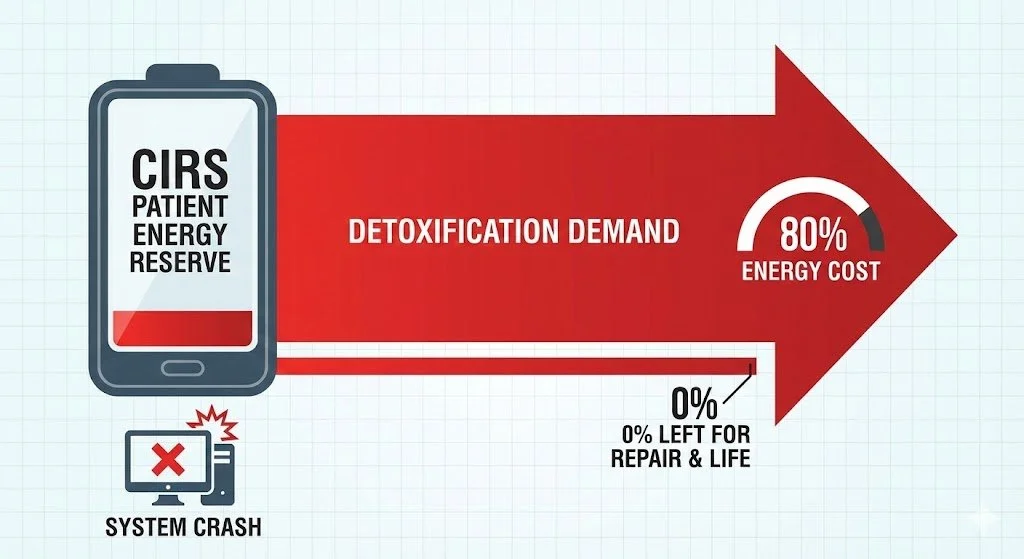
Restoring the Terrain in Mold Illness - Chronic Inflammatory Response Syndrome (CIRS): Beyond Functional Biochemical Detoxification
Chronic Inflammatory Response Syndrome (CIRS), commonly known as "Mold Illness," acquired from exposure to water-damaged buildings (WDB), represents a catastrophic failure of the innate immune system and cellular bioenergetics. The current integrative standard of care—Functional Medicine utilizing the Shoemaker Protocol—relies predominantly on biochemical interventions: systemic binders, targeted supplements, and dietary modulation to facilitate detoxification. While diagnostically precise and biochemically sound, this approach frequently encounters significant clinical ceilings in chronic, multisystemic cases. These limitations stem from a fundamental oversight: the inability of a metabolically exhausted host with compromised membrane transport and lymphatic stasis to execute complex biochemical detoxification pathways. This review argues for a paradigm shift toward a "Physics-First" hierarchy of care. By prioritizing advanced biophysical modalities—specifically Photobiomodulation (PBM), Hyperbaric Oxygen Therapy (HBOT) combined with Exercise with Oxygen Therapy (EWOT), Pulsed Electromagnetic Field (PEMF) therapy, and mechanical lymphatic/glymphatic clearance—clinicians can address the structural and energetic pathologies of CIRS that chemical agents cannot reach. We propose that restoring cellular voltage, reducing tissue hypoxia, and mechanically forcing detoxification pathways is the essential prerequisite for biochemical interventions to be effective.