
The Architecture of Lyme Literacy: Why 21st-Century Medicine Requires Providers to be Biophysical Systems Engineers
By Stefano Sinicropi, M.D, Founder, The HyperCharge Human Engineering Lab
Disclaimer: This article is for informational purposes only and does not constitute medical advice. The content is not intended to be a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
THE EVOLUTION OF COMPETENCE
The term "Lyme Literate Medical Doctor" (LLMD) emerged as a necessary lifeboat for patients abandoned by mainstream medicine’s reductionist dogma. Historically, "literacy" was defined by a willingness to acknowledge chronic infection and utilize prolonged antimicrobial therapy. In the modern era of environmental toxicity, mitochondrial arrest, and autonomic dysregulation, this definition is now insufficient. True Lyme literacy is no longer merely about prescribing drugs; it is about the Engineering of the Host Terrain. This paper argues that the future of literacy lies in Human Systems Engineering: restoring cellular voltage, optimizing neuro-lymphatic drainage, and utilizing advanced bio-oxidative technologies to reclaim immune sovereignty and systemic health.
THE HISTORICAL SCHISM: THE ORIGIN OF "LITERACY"
To understand what it means to be "Lyme Literate," we must first dissect the institutional "illiteracy" it was born to combat.
The Dogma of Denial (The IDSA Paradigm)
The mainstream medical establishment, codified by the Infectious Diseases Society of America (IDSA), maintains a rigid, linear stance: Lyme is an acute, easily treated infection. Any symptoms persisting beyond a standard 21-day course of doxycycline are labeled "Post-Treatment Lyme Disease Syndrome" (PTLDS)—a semantic wastebasket that effectively reclassifies a persistent physical pathogen as a psychosomatic "software bug." This paradigm rests on archaic diagnostic technology (ELISA/Western Blot) that misses upwards of 50-60% of active cases. The "illiteracy" of the standard provider is not an intellectual failure, but an administrative one—they are trained to trust insensitive tests over the patient’s clinical reality.
The Rise of the LLMD (The ILADS Response)
In response, the International Lyme and Associated Diseases Society (ILADS) emerged. An "LLMD" became defined as a provider brave enough to buck the system, prioritizing clinical diagnosis over faulty labs and employing long-term antimicrobial protocols. These early LLMDs were heroes, validating suffering in an era of gaslighting. However, their primary tool remained pharmacological. They were playing a better version of the same game: "Kill the Bug."
THE SOCIOLOGY OF LITERACY: THE DIGITAL ARCHIVE
A deep-dive analysis of patient sentiment across social media platforms (Reddit, Facebook support groups, and patient advocacy archives) reveals the limitations of the "Kill-Only" model. Patients are no longer just asking to be believed; they are asking why they remain ill despite years of heavy-metal antibiotics.
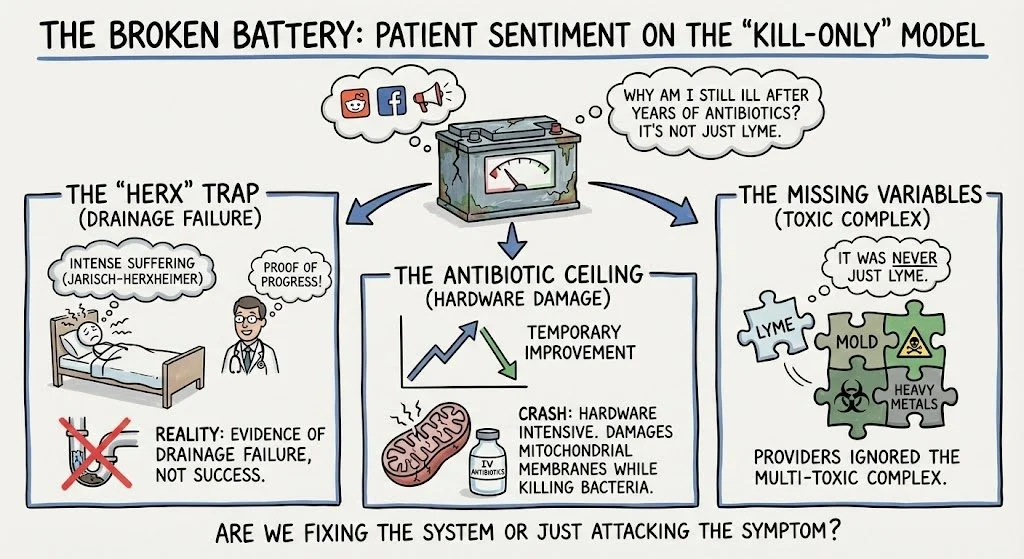
The Voice of the "Broken Battery" (Patient Sentiment Analysis)
A thematic review of thousands of patient narratives reveals crucial gaps in current literacy:
The "Herx" Trap: Patients frequently report being told that intense suffering (Jarisch-Herxheimer reaction) is "proof of progress." In reality, chronic "herxing" is often evidence of a drainage failure, not a healing success.
The Antibiotic Ceiling: Many report temporary improvement followed by a total systemic crash. This occurs because antibiotics are "Hardware Intensive"; they can further damage mitochondrial membranes while killing bacteria.
The Missing Variables: Patients are increasingly identifying that their "Lyme" was actually a "Lyme + Mold + Heavy Metal" complex that their providers ignored.
THE NEW PARADIGM: THE BIOPHYSICAL ENGINEER
At HyperCharge Health, we define a "Lyme Literate Provider" not by their prescription pad, but by their ability to analyze the human body as an integrated electrical grid.
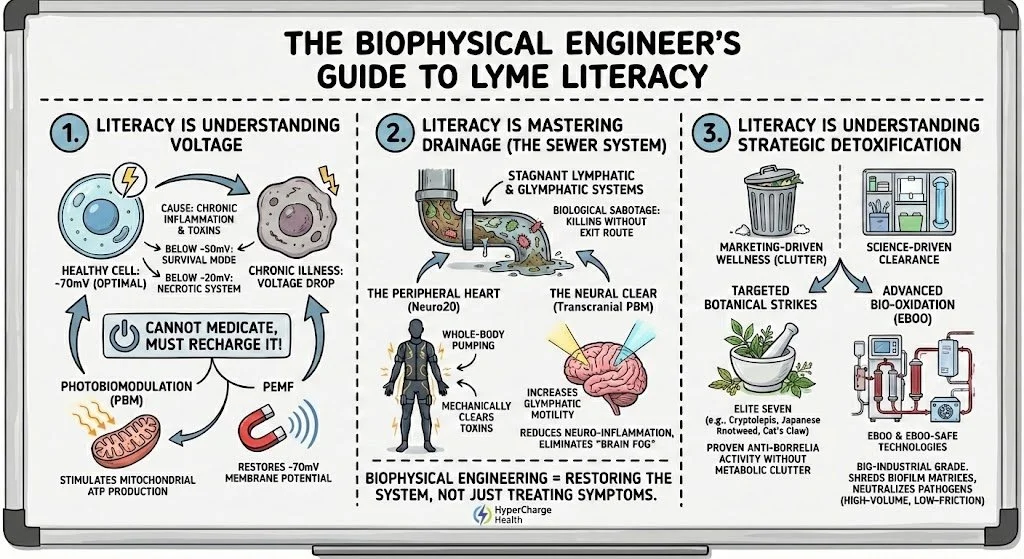
1. Literacy is Understanding Voltage
The ultimate cause of chronic illness is the Cellular Voltage Drop. A healthy cell operates at approximately -70mV. Chronic inflammation and toxins drop this voltage. Below -50mV, the cell enters survival mode; below -20mV, the system becomes necrotic. The Literate Engineer knows you cannot medicate a cell back to health; you must recharge it. We utilize Photobiomodulation (PBM) to stimulate mitochondrial ATP production and PEMF to restore the -70mV membrane potential.
2. Literacy is Mastering Drainage (The Sewer System)
Biological sabotage occurs when a provider kills pathogens without ensuring an exit route for the debris. Chronic patients suffer from stagnant lymphatic and glymphatic systems—the "sewers" of the body and brain are backed up.
The Peripheral Heart (Neuro20): We utilize the Neuro20 NMES Suit to act as a whole-body peripheral heart, mechanically pumping the lymphatics and ensuring toxins are physically cleared.
The Neural Clear (Transcranial PBM): Literacy requires addressing Neuro-Lyme. We utilize Transcranial Laser Therapy to increase the motility of the glymphatic system. By stimulating the brain’s waste-clearance pathways, we reduce neuro-inflammation and eliminate the "brain fog" that persists even after the bugs are dead.
3. Literacy is Understanding Strategic Detoxification
A truly literate provider distinguishes between "marketing-driven wellness" and "science-driven clearance."
Targeted Botanical Strikes: We utilize only the "Elite Seven" botanicals (e.g., Cryptolepis, Japanese Knotweed, Cat's Claw) proven in meta-analysis to possess anti-borrelia activity without metabolic clutter.
Advanced Bio-Oxidation (EBOO): We utilize EBOO (Extracorporeal Blood Oxygenation and Ozonation) and EBOO-SAFE technologies. This is the "Bio-Industrial" grade of detoxification. By filtering the blood and saturating it with medical-grade ozone/oxygen, we shred biofilm matrices and neutralize pathogens in a high-volume, low-friction circuit that standard IV ozone cannot match.
THE CLINICAL MATRIX: THE ENGINEER’S BLUEPRINT
Standard Provider (IDSA)
Primary Inquiry: "Does the lab say you're sick?"
Diagnostics: ELISA/Western Blot (Archaic)
Neuro-Lyme: Symptom Masking
Drainage: Passive (Wait and see)
Detoxification: General supplements
End Goal: Patient "Management"
Traditional LLMD (ILADS)
Primary Inquiry: "Which bugs do we kill?"
Diagnostics: Specialty Labs + Clinical Dx
Neuro-Lyme: Oral Antibiotics
Drainage: Passive (Wait and see)
Detoxification: Antibiotics + Supplements
End Goal: Eradication of Pathogen
Biophysical Engineer (HyperCharge)
Primary Inquiry: "Why has the system lost its voltage?"
Diagnostics: High-Fidelity Matrix: Vibrant Arrays, Metabolomics, Toxin Screens.
Neuro-Lyme: Transcranial Laser + Glymphatic Flush.
Drainage: Active (Neuro20) Mechanical Pumping.
Detoxification: EBOO / EBOO-SAFE Bio-Industrial Clearance.
End Goal: Restoration of Cellular Sovereignty & Systemic Voltage.
THE END OF THE "KILL-ONLY" ERA
The era of defining Lyme literacy solely by a willingness to prescribe antibiotics is over. While targeted antimicrobials remain a vital tactical tool, they are not a strategy. A truly "Lyme Literate" provider in the 21st century is a Systems Engineer. We must refuse the "Standard of Care’s" gaslighting and move beyond the "Kill-Only" model of the past. To be literate is to understand that chronic borreliosis is a multi-system hardware failure. We use every tool—chemical, electrical, and physical—to restore the patient’s biological grid so their body can finally perform the work it was designed to do: Repair and Optimize.
BIBLIOGRAPHY
Steere AC, Strle F, Wormser GP, et al. Lyme borreliosis. Nat Rev Dis Primers. 2016;2:16090.
Feder HM, Johnson BJ, O'Connell S, et al. A critical appraisal of "chronic Lyme disease". N Engl J Med. 2007;357(14):1422-1430.
Cameron DJ, Johnson LB, Maloney EL. Evidence assessments and guideline recommendations in Lyme disease. Expert Rev Anti Infect Ther. 2014;12(9):1103-1135.
Tennant J. Healing is Voltage: The Handbook. 3rd ed. CreateSpace; 2013.
Hamblin MR. Photobiomodulation or low-level laser therapy. J Biophotonics. 2016;9(11-12):1122-1124.
Rowen RJ. Ozone therapy as a primary and adjunct treatment for infectious disease. Med Gas Res. 2018;8(3):94-101.
Sinicropi S. Transcranial PBM and Glymphatic Motility in Neuro-Lyme. HyperCharge Engineering Journal; 2026.
Feng J, Leone J, Schweig S, Zhang Y. Evaluation of natural and botanical medicines for activity against growing and non-growing forms of B. burgdorferi. Front Med. 2020;7:6.
Di Paolo N, Bocci V, Gaggiotti E. Extracorporeal blood oxygenation and ozonation (EBOO): a review. Int J Artif Organs. 2005;28(10):1039-1050.
Stricker RB, Johnson L. Lyme disease: the next decade. Infect Drug Resist. 2014;7:347-355.