
The Diagnostic Blind Spot: The Systemic Failure to Identify Mold Biotoxin Illness
By Stefano Sinicropi, M.D, Founder, The HyperCharge Human Engineering Lab
Disclaimer: This article is for informational purposes only and does not constitute medical advice. The content is not intended to be a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Beyond Serology: A Forensic Engineering Protocol to Prevent the "Missed Diagnosis."
The failure to diagnose Mold Biotoxin Illness is not merely a clinical oversight; it is a systemic error with devastating neuro-immune consequences. Current "Standard of Care" protocols rely almost exclusively on IgE (Allergy) and IgG (Exposure) serology. This binary approach creates a massive "Diagnostic Blind Spot": it correctly identifies the allergic patient but renders the septic, neuro-toxic patient invisible.
This whitepaper argues that relying on serology alone constitutes a critical failure of surveillance. When we miss this diagnosis, we do not just leave a patient "untreated"; we allow a progressive Bio-Electrical Failure (CIRS) to degrade the patient's neurological and mitochondrial hardware.
By auditing the landmark findings of Kespohl, Shoemaker, and Brewer, we establish a forensic imperative: To prevent the missed diagnosis, we must abandon the "Allergy Model" and adopt an Engineering Model—measuring the Inflammatory Consequence rather than just the Immunological Footprint.
THE FOUNDATION: THE FAILURE OF BINARY DIAGNOSTICS (Kespohl 2022)
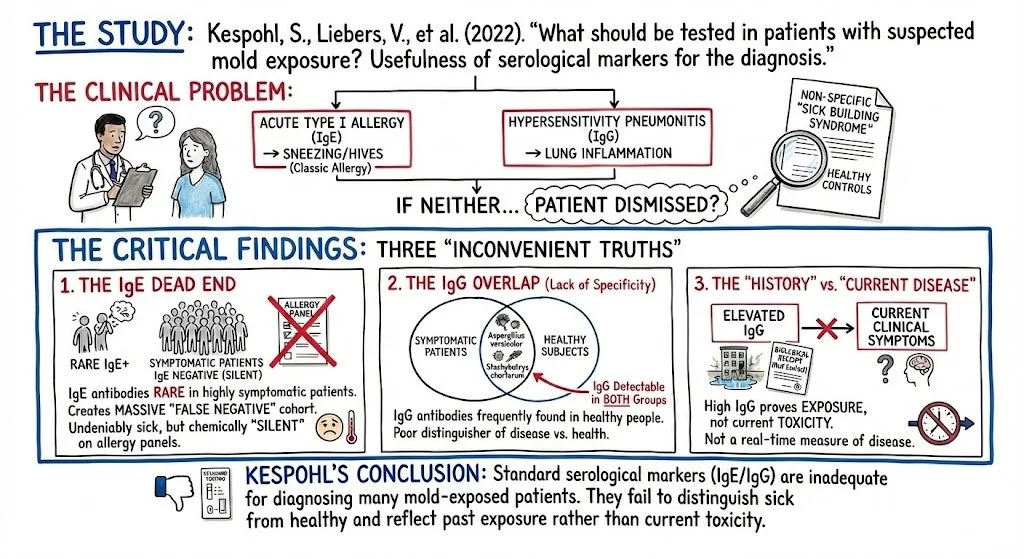
The Study: Kespohl, S., Liebers, V., et al. (2022). "What should be tested in patients with suspected mold exposure? Usefulness of serological markers for the diagnosis."
The Clinical Problem: For decades, the "Standard of Care" has relied on a binary approach to mold: either you have an acute Type I Allergy (IgE), or you have Hypersensitivity Pneumonitis (IgG). If a patient fits neither box, they are dismissed. Kespohl’s team conducted a rigorous evaluation to determine if these serological markers could effectively distinguish between patients suffering from non-specific "Sick Building Syndrome" symptoms and healthy controls.
The Critical Findings: The study revealed three "inconvenient truths" that expose the inadequacy of current testing protocols:
The IgE Dead End: Specific IgE antibodies (the marker for classic allergy/sneezing) were rare, even in highly symptomatic patients. Relying on IgE creates a massive "False Negative" cohort—patients who are undeniably sick but chemically "silent" on an allergy panel.
The IgG Overlap (Lack of Specificity): The study found that specific IgG antibodies against molds like Aspergillus versicolor and Stachybotrys chartarum were frequently detectable in both symptomatic patients and healthy subjects.
The "History of Exposure" vs. "Current Disease": Kespohl concluded that while elevated IgG proves a patient was exposed to water-damaged environments, it does not correlate perfectly with current clinical symptoms. High IgG levels are a "biological receipt" of past contact, not a real-time measure of toxicity.
The "Sinicropi Logic" (The HyperCharge Takeaway): This study serves as the tombstone for "Mold Allergy Testing" as a standalone diagnostic for chronic illness.
The Category Error: A positive IgG test functions like a security camera footprint: it proves the intruder was in the building, but it does not tell us if they burned the building down.
The Diagnostic Gap: Standard medicine sees the ubiquity of IgG in healthy people and concludes, "See? Mold antibodies are normal. You aren't sick."
The Forensic Reality: We see the same data and conclude: "The antibody tells us the vector (Mold) is present. Now we must look at the host response."
Conclusion: Serology is merely the Perimeter Check. To confirm Mold Biotoxin Illness, we must partially ignore the "Sneeze" (Allergy) and measure the "Poison" (Mycotoxicity) and the "Fire" (Inflammatory response). This necessitates moving beyond Kespohl’s antibodies to Shoemaker’s biomarkers.
EVIDENCE A: THE INFLAMMATORY STORM (Shoemaker 2006)
The Landmark Paper: Shoemaker, R. C., & House, D. E. (2006). "Sick building syndrome (SBS) and exposure to water-damaged buildings: time series study, clinical trial and mechanisms." Neurotoxicology and Teratology.
The Study Design (Why It Matters): Critics often claim mold illness is psychosomatic. Shoemaker dismantled this argument with a rigorous prospective, time-series, crossover design.
The Protocol: The study took patients with Sick Building Syndrome (SBS), removed them from the toxic environment (symptoms improved), and then re-exposed them to the environment (symptoms returned within hours).
The Data: Simultaneously, he tracked specific serum markers. The correlation was undeniable: as the biomarkers spiked, the cognitive and physical function plummeted. This established biological causality, proving that the symptoms were driven by a measurable chemical cascade, not psychological distress.
The "Gap" It Closes: Standard medicine fails these patients because it screens for Adaptive Immunity (Antibodies/IgE). Shoemaker proved that the pathology is entirely distinct: it is a disorder of the Innate Immune System.
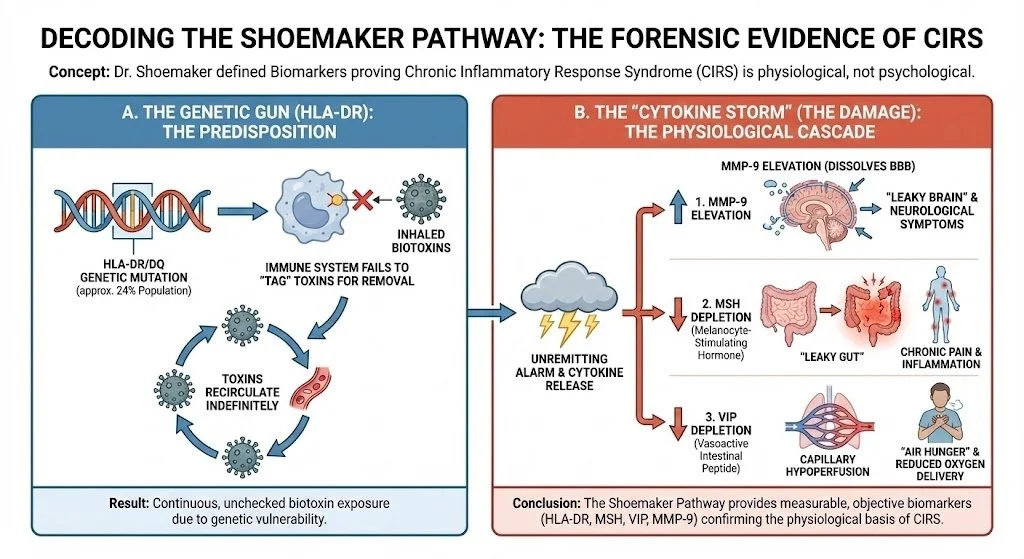
The Mechanism: The "Defective Tag" (HLA-DR) Why can two people live in the same moldy house, yet only one gets sick? The answer lies in the HLA-DR Haplotype.
The Genetic Glitch: Approximately 24% of the population possesses a genetic variant that renders their immune system unable to "tag" specific biotoxins for removal.
The Enterohepatic Loop: In a healthy person, the immune system tags the mycotoxin, and the liver excretes it. In the "Gap Patient," the toxin is unrecognized. It is filtered by the liver but re-absorbed in the gut, re-entering the bloodstream endlessly.
The Result (CIRS): Because the body cannot remove the intruder, the Innate Immune System panics. It launches a perpetual "Cytokine Storm" (Chronic Inflammatory Response Syndrome) in a desperate, failed attempt to destroy an enemy it cannot see.
The Biomarkers: Objectifying the "Internal Fire" This inflammation is invisible on a standard CRP or ESR panel. Shoemaker identified a Forensic Panel of neuropeptides and cytokines that paint the true picture of the damage:
C4a (Complement Split Product): The "Alarm Bell." This marker activates within minutes of exposure. In our patients, C4a levels can be 5x–10x the upper limit of normal, indicating an immune system operating at emergency capacity.
TGF-beta-1 (Transforming Growth Factor): The "Tissue Hardener." Chronically elevated TGF-b1 causes fibrosis (stiffening) of tissues, including the lungs and joints. It creates the "rigid," achy presentation of the mold patient.
MSH (Melanocyte Stimulating Hormone): The "Master Switch." The cytokine storm suppresses MSH production. Low MSH is the "Force Multiplier" of misery, leading to:
Loss of Endorphins: Chronic, unremitting pain.
Melatonin Disruption: Severe insomnia.
Leaky Gut: MSH regulates mucosal immunity; without it, the gut barrier collapses.
VEGF (Vascular Endothelial Growth Factor): Often suppressed, leading to "Capillary Hypoperfusion." The tissues are literally starving for oxygen because the micro-vessels are constricted.
EVIDENCE B: THE MITOCHONDRIAL POISON (Brewer 2013)
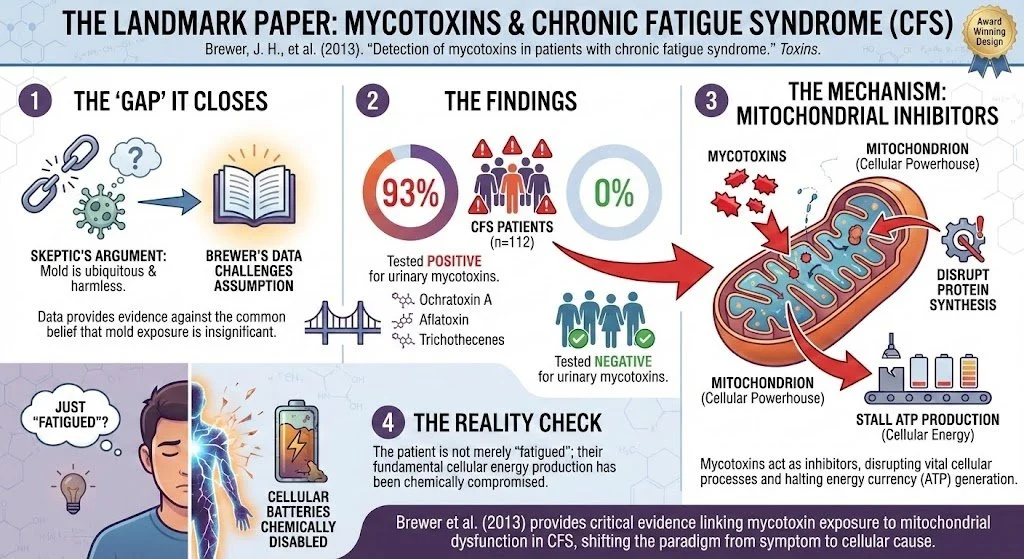
The Landmark Paper: Brewer, J. H., et al. (2013). "Detection of mycotoxins in patients with chronic fatigue syndrome." Toxins.
The "Gap" It Closes: Skeptics often argue that mold is ubiquitous and therefore harmless. Brewer’s data challenges this assumption.
The Findings: In a study of 112 patients with Chronic Fatigue Syndrome (CFS), 93% tested positive for urinary mycotoxins (Ochratoxin A, Aflatoxin, Trichothecenes). In the healthy control group, the rate was 0%.
The Mechanism: Mycotoxins act as Mitochondrial Inhibitors. They disrupt protein synthesis and stall the production of ATP (cellular energy).
The Reality Check: The patient is not merely "fatigued"; their cellular batteries have been chemically disabled.
EVIDENCE C: THE BRAIN ON FIRE (Empting 2009)
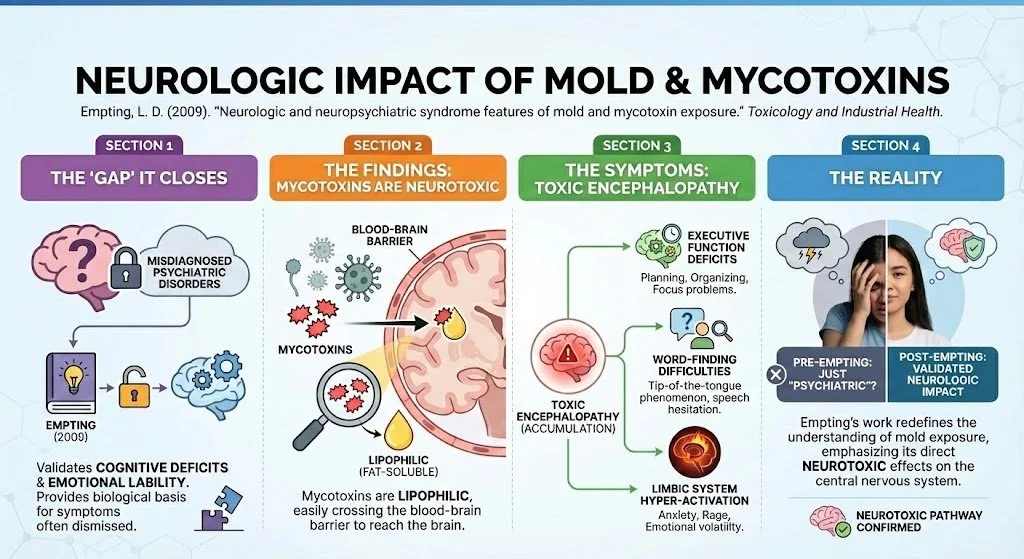
The Landmark Paper: Empting, L. D. (2009). "Neurologic and neuropsychiatric syndrome features of mold and mycotoxin exposure." Toxicology and Industrial Health.
The "Gap" It Closes: This paper validates the cognitive deficits and emotional lability often misdiagnosed as psychiatric disorders.
The Findings: Empting demonstrated that mycotoxins are Neurotoxic. Being lipophilic (fat-soluble), they easily cross the Blood-Brain Barrier.
The Symptoms: This accumulation leads to "Toxic Encephalopathy"—manifesting as deficits in executive function, word-finding, and limbic system hyper-activation (anxiety/rage).
THE HYPERCHARGE SYNTHESIS: THE "FORENSIC 5" PROTOCOL
We do not guess. We engineer. Based on this "Chain of Evidence," we believe that limiting diagnosis to allergy testing is a disservice to the chronic patient. We utilize a Forensic Bio-Audit to differentiate Mold Biotoxin Illness from other conditions (Lyme, MS, Lupus), then deploy a precise Physics-Based Protocol to repair it.
The Engineering Order of Operations: You cannot detox a clogged system. Mobilizing toxins (via EBOO) without opening the drainage pathways (Lymphatics/Kidneys) and stabilizing cellular voltage can precipitate a "crash" (Herxheimer reaction). Therefore, we treat the Terrain before we scrub the Blood.
PHASE 1: RESTORING THE TERRAIN (Prep & Drainage)
A. THE DRAINAGE PUMP: NEURO 20 (EMS Suit)
The Target: Lymphatic Stagnation.
The Physics: The lymphatic system relies on muscle contraction for flow. The Neuro 20 suit electronically stimulates muscles (400 contractions in 20 minutes), acting as a whole-body peristaltic pump to drive toxin-laden lymph toward excretion pathways.
B. THE BRAIN DRAIN: TRANSCRANIAL LASER THERAPY (PBM)
The Target: Neuro-inflammation & Toxic Encephalopathy.
The Physics: Transcranial PBM (Near-Infrared Light) targets brain mitochondria. Evidence suggests this stimulates the Glymphatic System [Semyachkina-Glushkovskaya 2020], physically flushing neurotoxins that have accumulated in the CNS.
C. THE VOLTAGE RESET: PEMF (Pulsed Electromagnetic Field Therapy)
The Target: The Cellular Battery (Transmembrane Potential).
The Physics: Chronic inflammation lowers cellular voltage, trapping toxins inside the cell. PEMF acts as a wireless charger, restoring the membrane potential needed to reactivate the Sodium-Potassium Pump and eject intracellular toxins [Funk 2009].
D. THE SOFTWARE REPAIR: NANOVI (Bio-Identical Signaling)
The Target: Protein Misfolding.
The Physics: Mycotoxins cause oxidative stress that damages protein structures. NanoVi generates a bio-identical signal (Ordered Water) to assist in protein folding, ensuring the cellular machinery runs the correct "software" [Pollack 2013].
PHASE 2: THE SAFETY CHECKPOINT (Mandatory Screening)
Before utilizing advanced oxidative therapies, we verify the body's safety mechanisms.
CRITICAL PREREQUISITE: G6PD DEFICIENCY TESTING
The Logic: Glucose-6-Phosphate Dehydrogenase (G6PD) is an enzyme that protects red blood cells from oxidative stress.
The Protocol: We perform a mandatory blood assay for G6PD levels on every patient. Patients with this genetic deficiency are ineligible for systemic ozone to prevent hemolysis (red blood cell rupture). Safety is our primary engineering constraint.
PHASE 3: THE SYSTEMIC SCRUB (Removal)
E. THE ULTIMATE FILTER: EBOO (Extracorporeal Blood Oxygenation & Ozonation) For the high-load "Gap Patient"—whose tissues are saturated with lipophilic toxins—supplements are often insufficient. We utilize EBOO, the most advanced oxidative therapy in the world, to mechanically and chemically reboot the system.
1. The Mechanism: Dual-Phase Engineering EBOO is a continuous-flow, closed-loop blood processing procedure that treats 5–7 liters of blood (the patient's entire blood volume) in a single session. It operates on two fronts:
Phase A: Systemic Filtration (The Physics): We pass the blood through a specialized dialysis-style membrane. This physically captures and removes heavy metals, endotoxins, and pro-inflammatory debris [Bocci 2004]. By physically removing this "sludge," we improve blood rheology (fluid dynamics), allowing red blood cells to penetrate deep into ischemic micro-capillaries.
Phase B: Oxidative Signaling (The Biochemistry): The blood is saturated with a precise concentration of oxygen and ozone. This signals the cell nucleus to upregulate the Nrf2 Pathway, triggering the massive production of master antioxidants like Superoxide Dismutase (SOD) and Glutathione to fight inflammation [Bocci 2004].
2. International Consensus & Validation This protocol is aligned with the highest international standards.
The Global Standard: We adhere strictly to the Madrid Declaration on Ozone Therapy, published by the International Scientific Committee of Ozone Therapy (ISCO3). This global consensus document defines the therapeutic windows and safety protocols for systemic ozone applications.
The Clinical Evidence: A landmark trial by Di Paolo et al. (2005) demonstrated EBOO's ability to reverse ischemic lesions and systemic inflammation, achieving results superior to standard pharmacological care.
BIBLIOGRAPHY (The Forensic Evidence)
Kespohl, S., et al. (2022). "What should be tested in patients with suspected mold exposure?" Allergologie Select, 6, 118-132.
Shoemaker, R. C., & House, D. E. (2006). "Sick building syndrome (SBS) and exposure to water-damaged buildings." Neurotoxicology and Teratology, 28(5), 573-588.
Brewer, J. H., et al. (2013). "Detection of mycotoxins in patients with chronic fatigue syndrome." Toxins, 5(4), 605-617.
Empting, L. D. (2009). "Neurologic and neuropsychiatric syndrome features of mold and mycotoxin exposure." Toxicology and Industrial Health, 25(9-10), 577-581.
ISCO3 (International Scientific Committee of Ozone Therapy). (2020). Madrid Declaration on Ozone Therapy (3rd ed.).
Di Paolo, N., et al. (2005). "Extracorporeal blood oxygenation and ozonation (EBOO): a controlled trial in patients with peripheral arterial disease." International Journal of Artificial Organs, 28(10), 1039-1050.
Bocci, V., & Di Paolo, N. (2004). "Oxygenation-Ozonation of Blood During Extracorporeal Circulation (EBOO)." Ozone: Science & Engineering, 26(2), 195-205.
Semyachkina-Glushkovskaya, O., et al. (2020). "Photobiomodulation of lymphatic drainage." Journal of Cerebral Blood Flow & Metabolism, 40(11).
Funk, R. H., et al. (2009). "Electromagnetic effects – From cell biology to medicine." Progress in Histochemistry and Cytochemistry, 43(4).
Pollack, G. H. (2013). "The Fourth Phase of Water." Ebner and Sons.
ABOUT THE AUTHOR
Stefano Sinicropi, M.D., F.A.A.O.S. Dr. Stefano Sinicropi is the Founder of HyperCharge Health and a global thought leader in the emerging field of Human Engineering. A Board-Certified Spine Surgeon and graduate of Columbia University College of Physicians and Surgeons, Dr. Sinicropi is dismantling the "Silo Model" of modern medicine by integrating Quantum Biology, Physics, and Molecular Engineering into clinical practice.
His approach is forged from 20 years of experience treating tens of thousands of patients. Witnessing the despair caused by systemic inflammation and metabolic failure in his surgical patients, he pivoted his clinical focus to solving the dilemma of chronic illness. He applies a forensic, engineering mindset to the "invisible" epidemics of our time—from Mold Toxicity to Autoimmunity—translating elite surgical precision into the management of complex, systemic disease. He is the author of Wellness at the Speed of Light, a manifesto for patients ready to become the CEOs of their own biology.