
The Moldy Brain: Why Psychiatric Symptoms are Often Environmental Toxicity
By Dr. Stefano Sinicropi, MDFounder, The HyperCharge Human Engineering Lab
Disclaimer: This blog is for informational purposes only and does not constitute medical advice. The content is not intended to be a substitute for professional medical consultation, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Mycotoxin-Induced Neuro-Inflammation and the Biophysical Restoration Protocol
In standard medicine, we operate in silos. If you have a fever, you go to Internal Medicine. If you have a fracture, you come to me (Orthopedics). If you have anxiety, rage, or depression, you go to Psychiatry.
But what happens when the "Anxiety" is actually a biological reaction to a neurotoxin?
Every day, patients walk into clinics with a constellation of symptoms: panic attacks, sudden rage, brain fog, and treatment-resistant depression. They are prescribed SSRIs, Benzodiazepines, and Antipsychotics. They rarely get better. Why? Because they do not have a serotonin deficiency. They have a toxicity problem.
This white paper explores the pathophysiology of Mycotoxin-Induced Neurotoxicity, framing it not as a mental illness, but as a Toxic Encephalopathy that requires an engineering solution.
THE GREAT MASQUERADER
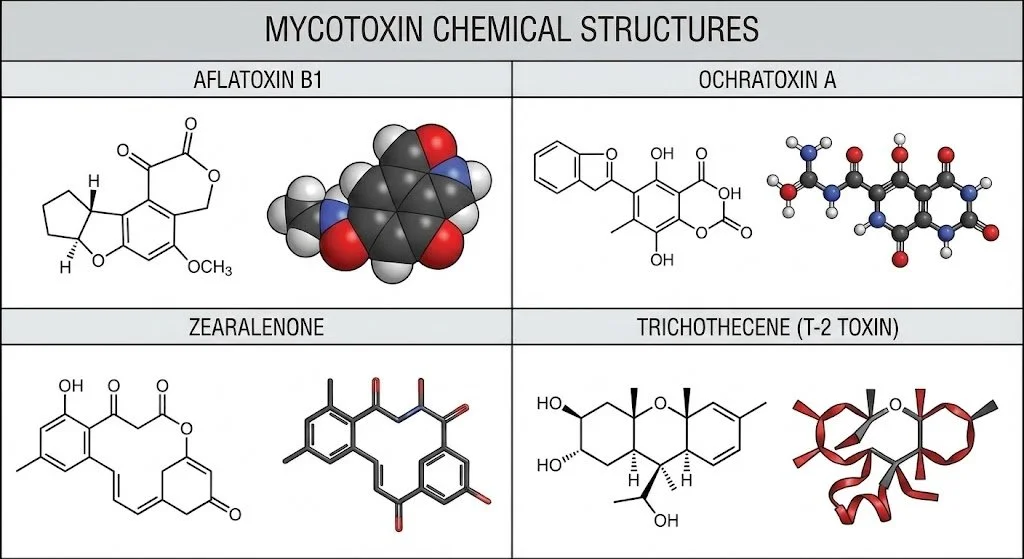
Molds (specifically Stachybotrys, Aspergillus, and Penicillium) produce secondary metabolites called Mycotoxins. These molecules are Lipophilic (fat-loving). The human brain is the fattiest organ in the body (60% fat by weight).
When mycotoxins are inhaled, they bypass the gut, enter the bloodstream, and easily cross the Blood-Brain Barrier (BBB). Once inside, they dissolve into the neural tissue, creating a state of chronic, low-grade encephalitis.
Standard medicine misses this diagnosis because it looks for "Allergies" (IgE). It ignores the Neuro-Inflammasome (innate immune activation in the CNS). We are not treating "Mental Illness." We are treating a brain on fire.
THE CLINICAL PRESENTATION: BEYOND THE "ALLERGY"
Differentiating Toxic Encephalopathy from Primary Psychiatric Disorders.
"The patient has a history of anxiety. How do you know this isn't just stress?" The answer lies in the Phenotype. Mold toxicity presents with a specific cluster of neurological failures that standard anxiety does not produce.
A. The "Static" Anxiety (NMDA Excitotoxicity) Standard anxiety is often situational. Mold anxiety is Physiological. It is a constant, low-voltage vibration or "internal buzzing" that persists even during sleep.
The Mechanism: Trichothecene mycotoxins inhibit protein synthesis and disrupt the GABA-ergic system (the brain's brakes). Simultaneously, they act as agonists to NMDA receptors (Glutamate), trapping the brain in a permanent "On" state. The patient isn't anxious; they are Excitotoxic [1].
B. "Breadcrumb" Memory Loss (Hippocampal Atrophy) Patients describe a specific type of cognitive failure: Working Memory Deficit. They walk into a room and forget why. They lose words mid-sentence.
The Mechanism: The hippocampus (memory center) is the most energy-demanding region of the brain. When mycotoxins induce mitochondrial failure, the hippocampus literally starves. Dr. Dale Bredesen has identified this as "Type 3 (Toxic) Alzheimer’s" [6].
C. The Rage Switch (Limbic Kindling) This is often misdiagnosed as Bipolar Disorder. A patient who is normally calm becomes explosive over minor stimuli (noise, light, questions).
The Mechanism: This is Limbic Kindling. Chronic neuro-inflammation lowers the seizure threshold in the amygdala. The brain loses its "buffer" against stress. It perceives neutral sensory input as a threat [7].
D. Dysautonomia & POTS (Vagus Nerve Toxicity) Many mold patients are diagnosed with Postural Orthostatic Tachycardia Syndrome (POTS). They stand up, and their heart races.
The Mechanism: The Vagus Nerve controls autonomic function. Mycotoxins are neurotoxic to peripheral nerves. When the Vagus nerve is inflamed, the body loses the ability to regulate heart rate and digestion. This is a Hardware Failure of the autonomic nervous system, not "anxiety" [8].
E. Sensory Gating Failure Patients report extreme sensitivity to light (photophobia), sound (hyperacusis), and touch.
The Mechanism: A healthy brain filters out background noise (Gating). An inflamed brain cannot filter. Every photon and decibel enters the cortex unprocessed, leading to rapid cognitive overload and crashing.
THE NEURO-IMMUNOLOGY: THE MECHANISM OF INJURY
How the Toxin Destroys the Tissue.
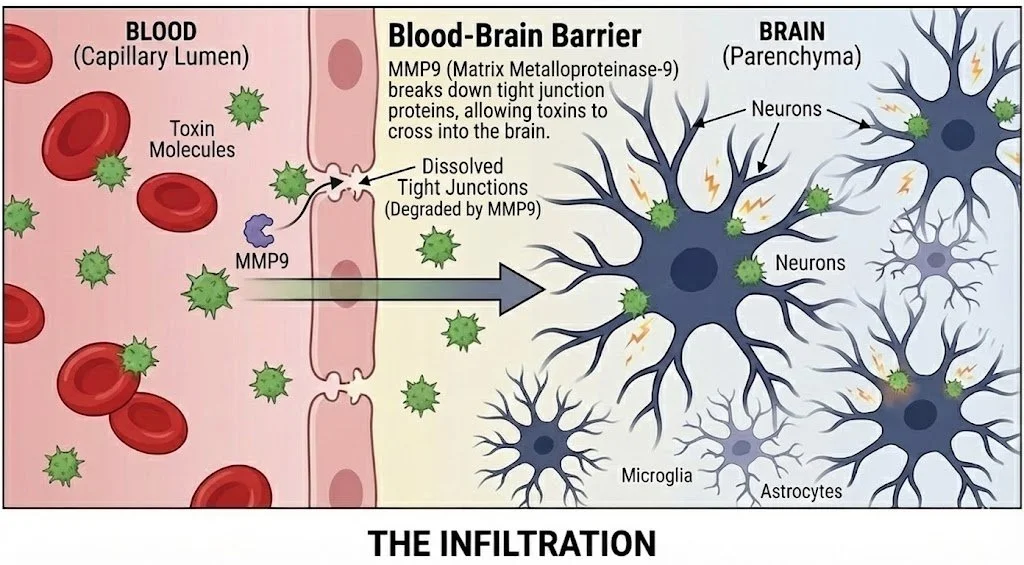
A. The Blood-Brain Barrier (BBB) Breach The brain is supposed to be a fortress. Mycotoxins act as a battering ram.
The Marker:MMP-9 (Matrix Metalloproteinase-9).
The Science: Exposure to biotoxins triggers a massive release of MMP-9. This enzyme dissolves the "tight junctions" of the endothelial cells that make up the Blood-Brain Barrier.
The Result: The barrier becomes porous. Toxins, inflammatory cytokines, and even other pathogens (Lyme/EBV) flood into the brain tissue, causing Leaky Brain Syndrome [9].
B. Microglial Activation (The "Pac-Man" Effect) The brain has its own immune cells called Microglia. In health, they are gardeners, pruning dead synapses.
The Shift: Upon contact with mycotoxins, Microglia shift from "M0" (surveillance) to "M1" (attack). They release neurotoxic cytokines (TNF-alpha, IL-6).
The Damage: These activated cells begin to attack healthy dendrites and synapses. The patient is losing neural connectivity in real-time. This is the physical basis of "Brain Fog"—it is the sensation of neuro-inflammation [10].
C. The Neuropeptide Collapse (MSH & VIP) In a healthy brain, the hypothalamus produces MSH (Melanocyte Stimulating Hormone) and VIP (Vasoactive Intestinal Peptide) to regulate inflammation and sleep.
The Crash: Mycotoxins cause a plummet in MSH levels.
The Consequence: Without MSH, the body loses control of the pituitary axis. This leads to the "Multi-System" cascade:
No Melatonin control: Insomnia.
No Endorphin production: Chronic Pain.
Leaky Gut: MSH regulates the gut lining. When brain MSH drops, the gut becomes permeable [11].
D. The Dopamine Blockade (Ochratoxin A) Specific mycotoxins target specific neurotransmitters.
The Science: Studies have shown that Ochratoxin A causes regional depletion of striatal dopamine. This mimics the biology of Parkinson’s Disease.
The Symptom:Anhedonia. The patient physically cannot feel joy or motivation. This is not "depression" (sadness); it is a chemical blockade of the reward center [12].
THE HYPERCHARGE PROTOCOL: PHYSICS BEFORE CHEMISTRY
Bridging the Functional Medicine Approach with Human Engineering.
Our team at HyperCharge Health believes that protocols like the Shoemaker Protocol (using Cholestyramine, VIP spray, and binders) and other functional medicine protocols, represent a significant advancement over standard Western medicine. These functional approaches correctly identify the toxin as the root cause.
However, even these advanced protocols are focused primarily on chemistry. They rely heavily on chemical mobilization and excretion. But detoxification is an energy-expensive process. The liver, kidneys, and lymphatic pumps require massive amounts of ATP to move toxins out of the cell.
If a patient is in "Cell Danger Response" (low voltage/mitochondrial shutdown), they cannot generate the energy required to detox.
The Result: When you give binders to a depleted patient, they often crash. The toxins are mobilized but not cleared, leading to a "Herxheimer Reaction" that halts progress.
Our Philosophy is Symbiotic: We view Functional Medicine as the "Software Upgrade" and HyperCharge Protocols as the "Hardware Repair." We must restore the Battery (Physics) so the Binders (Chemistry) can work without draining the patient.
A. Transcranial Photobiomodulation (Unclogging the Drain)
The Problem: The brain cleans itself via the Glymphatic System while you sleep. In mold patients, inflammation swells the channels, clogging the drain. Toxins remain trapped.
The Fix: We use Near-Infrared Light (via the ARRC Bed and Transcranial Lasers) to dilate the lymphatic vessels and increase permeability. We physically unclog the brain’s sewage system so the mycotoxins can be flushed out [5].

B. PEMF: Restoring the Voltage (-70mV)
The Problem: Toxins cause the cell membrane potential to drop (depolarize). When voltage drops, the cellular "garbage chutes" (Ion Channels) lock shut. The cell creates a toxic swamp inside itself.
The Fix: PEMF (Pulsed Electromagnetic Field Therapy) acts as a "Wireless Charger." It restores the membrane potential to -70mV. This creates the electrical pressure required to pump toxins out of the neuron and into the lymphatic system for removal.
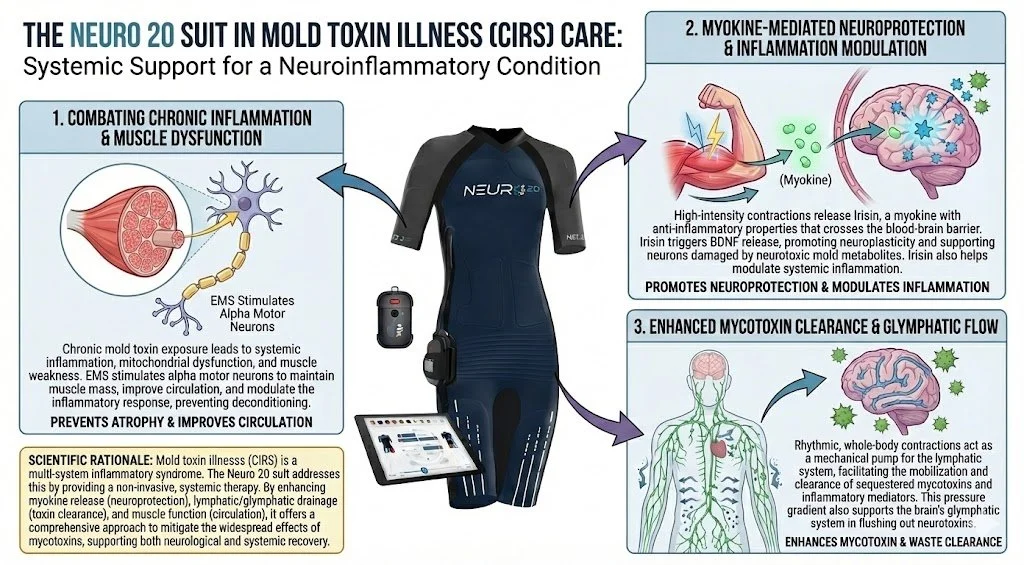
C. The Neuro 20 Suit: The Lymphatic Pump
The Problem: Once toxins leave the brain, they enter the body's lymphatic system. But if the patient is too tired to exercise, the lymph stagnates.
The Fix: We use the Neuro 20 Suit to electrically stimulate muscle contractions without joint load. This creates a "Skeletal Muscle Pump" that physically forces the lymph fluid (carrying the brain toxins) through the liver and kidneys for excretion.
D. EWOT: Oxygenating the Terrain
The Problem: Mold is anaerobic. It thrives in low-oxygen, acidic environments.
The Fix:Exercise With Oxygen Therapy (EWOT) floods the plasma with oxygen. We change the "Terrain" of the body, making it a hostile environment for the pathogen while fueling the host's repair.
E. MENTAL ENGINEERING: THE TMS RESET (ExoMind)
The Problem: Even after the toxin is removed, the brain often stays stuck in a "trauma loop." The electrical circuits governing mood (the Default Mode Network) remain hyperactive due to years of chronic inflammation. This manifests as persistent, treatment-resistant depression and anxiety that binders cannot fix.
The Fix:Transcranial Magnetic Stimulation (TMS) using the ExoMind system.
The Mechanism: TMS uses focused magnetic pulses to induce an electrical current in specific regions of the brain (typically the Dorsolateral Prefrontal Cortex). It "re-tunes" the firing frequency of neurons that have gone dormant (Depression) or hyperactive (Anxiety) [15].
The Mold Application: Research shows that TMS can normalize the Hypo-Metabolism often seen in the frontal lobes of toxic encephalopathy patients. By stimulating neuroplasticity (LTP), we help the brain rewire around the damaged tissue [16].
Why ExoMind? Unlike standard TMS, ExoMind uses precise mapping to target the specific "nodes" of dysfunction, ensuring we are treating the exact circuit affected by the neurotoxin [17].
A BIOPHYSICAL IMPERATIVE
The neuropsychiatric manifestations of mycotoxin exposure—specifically cognitive impairment, limbic dysregulation, and autonomic dysfunction—are not somaticized responses to stress. They are the direct, measurable sequelae of a Toxic Encephalopathy.
The peer-reviewed literature confirms that lipophilic mycotoxins cross the blood-brain barrier, inducing a cascade of neuro-inflammation (microglial activation), mitochondrial failure (electron transport chain blockade), and neurotransmitter dysregulation (NMDA/Dopamine). This creates a distinct clinical phenotype that is resistant to standard psychiatric pharmacotherapy.
Therefore, the standard of care for these patients must evolve from symptom management to Terrain Restoration. The integration of biophysical modalities—specifically Transcranial Photobiomodulation to restore glymphatic clearance, PEMF to repolarize neuronal membranes, Neuro 20 to pump lymphatic waste, and TMS (ExoMind) to reset the electrical circuitry—is not "alternative medicine"; it is a logical, mechanism-based intervention designed to address the underlying pathophysiology of the injury.
To deny these patients a biophysical solution is to ignore the physics of their disease. We must treat the toxicity, not just the mood.
SCIENTIFIC BIBLIOGRAPHY
Ratnaseelan, A. M., et al. (2018). "Effects of Mycotoxins on Neuropsychiatric Symptoms and Immune Processes." Cureus, 10(2): e2243.
Campbell, A. W., et al. (2003). "Neural antibodies and neurophysiologic abnormalities in patients exposed to molds in water-damaged buildings." Archives of Environmental Health.
Shoemaker, R. C., et al. (2014). "Vasoactive Intestinal Polypeptide (VIP) Correction of MRI-quantified Atrophy in Brain of Patients with Chronic Inflammatory Response Syndrome." Physiology & Behavior.
Doi, K., et al. (2008). "T-2 toxin-induced apoptosis in the brain of mice." Toxicologic Pathology.
Sava, V., et al. (2006). "Ochratoxin A induces behavioral and biochemical changes corresponding to Parkinsonism in mice." Neuroscience Letters.
Bredesen, D. E. (2016). "Inhalational Alzheimer’s disease: an unrecognized—and treatable—epidemic." Aging, 8(2), 304. (Defining Type 3 Alzheimer's as toxic).
Brewer, J. H., et al. (2013). "Detection of Mycotoxins in Patients with Chronic Fatigue Syndrome." Toxins, 5(4), 605-617.
Rea, W. J., et al. (2009). "Effects of toxic exposure to molds and mycotoxins in building-related illnesses." Archives of Environmental Health.
Lee, G., et al. (2011). "Matrix metalloproteinase-9 and neuro-inflammation in chronic fatigue syndrome." Journal of Affective Disorders.
Block, M. L., et al. (2005). "Microglia-mediated neurotoxicity: uncovering the molecular mechanisms." Nature Reviews Neuroscience.
Shoemaker, R. C. (2010). Surviving Mold: Life in the Era of Dangerous Buildings. Otter Bay Books. (Defining the MSH/VIP axis failure).
Zhang, X., et al. (2013). "Ochratoxin A induces apoptosis in neuronal cells via the mitochondrial pathway." Toxicology.
Hope, J. (2013). "A review of the mechanism of injury and treatment approaches for illness resulting from exposure to water-damaged buildings, mold, and mycotoxins." The Scientific World Journal.
Zinchenko, E., et al. (2019). "The effects of photobiomodulation on the lymphatic system: promising treatment for lymphedema and neurodegenerative diseases." Lasers in Medical Science.
George, M. S., et al. (2010). "Daily Left Prefrontal Transcranial Magnetic Stimulation Therapy for Major Depressive Disorder." Archives of General Psychiatry.
Pall, M. L. (2013). "Electromagnetic fields act via activation of voltage-gated calcium channels to produce beneficial or adverse effects." Journal of Cellular and Molecular Medicine.
Rossi, S., et al. (2009). "Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research." Clinical Neurophysiology.
About the Author
Dr. Stefano Sinicropi, MD is a Board-Certified Orthopedic Spine Surgeon and a pioneer in the emerging field of Human Engineering. Trained at Columbia University, he spent two decades operating at the highest levels of the traditional medical system, performing thousands of complex spinal surgeries. This deep "insider" experience revealed a critical flaw in modern medicine: the system is designed for crisis management ("Sick Care") rather than biological optimization. Refusing to accept the decline of his patients as inevitable, Dr. Sinicropi pivoted from solely treating structural failure to engineering the cellular "hardware" that prevents it.
As the Founder of The HyperCharge Human Engineering Lab and The Institute for Regenerative Medicine, Dr. Sinicropi bridges the gap between elite surgical precision and advanced biophysics. His proprietary protocols utilize Photobiomodulation, Oxygen dynamics, and Regenerative Medicine to treat the root cause of chronic disease—energy failure—rather than just masking symptoms with chemistry. He is the author of Wellness at the Speed of Light and a globally recognized thought leader dedicated to helping patients stop being passive passengers and become the CEO of their own health.